

Anabolic Resistance in the Pathogenesis of Sarcopenia in the Elderly: Role of Nutrition and Exercise in Young and Old People
- PMID: 37764858
- PMCID: PMC10535169
- DOI: 10.3390/nu15184073
Anabolic Resistance in the Pathogenesis of Sarcopenia in the Elderly: Role of Nutrition and Exercise in Young and Old People
Abstract
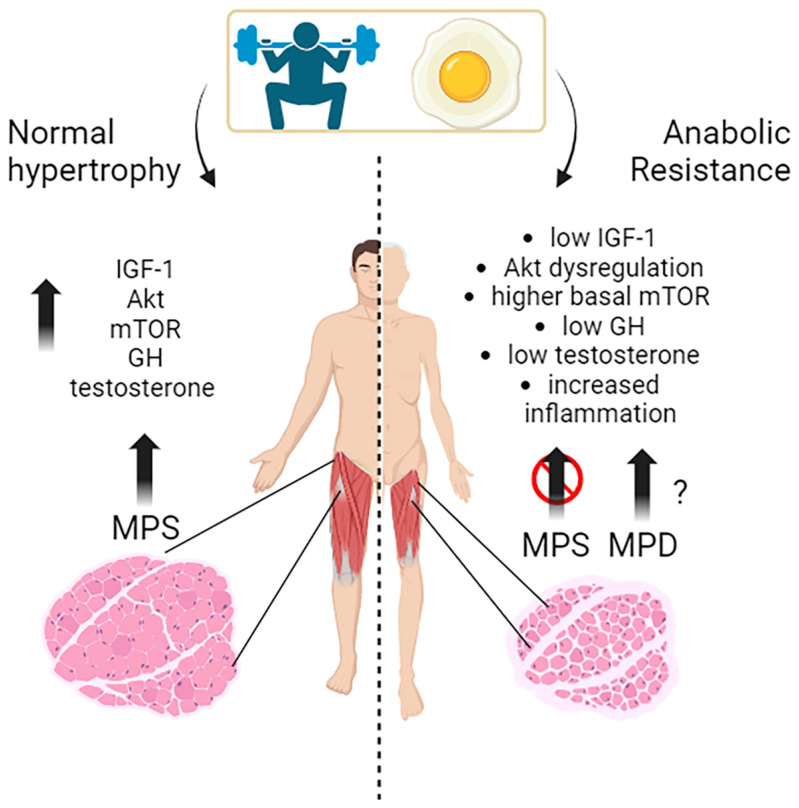
The development of sarcopenia in the elderly is associated with many potential factors and/or processes that impair the renovation and maintenance of skeletal muscle mass and strength as ageing progresses. Among them, a defect by skeletal muscle to respond to anabolic stimuli is to be considered. Common anabolic stimuli/signals in skeletal muscle are hormones (insulin, growth hormones, IGF-1, androgens, and β-agonists such epinephrine), substrates (amino acids such as protein precursors on top, but also glucose and fat, as source of energy), metabolites (such as β-agonists and HMB), various biochemical/intracellular mediators), physical exercise, neurogenic and immune-modulating factors, etc. Each of them may exhibit a reduced effect upon skeletal muscle in ageing. In this article, we overview the role of anabolic signals on muscle metabolism, as well as currently available evidence of resistance, at the skeletal muscle level, to anabolic factors, from both in vitro and in vivo studies. Some indications on how to augment the effects of anabolic signals on skeletal muscle are provided.
Keywords: exercise; intracellular signals; nutrition; protein foods; protein synthesis; sarcopenia; skeletal muscle.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Dent E., Morley J.E., Cruz-Jentoft A.J., Arai H., Kritchevsky S.B., Guralnik J., Bauer J.M., Pahor M., Clark B.C., Cesari M., et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging. 2018;22:1148–1161. doi: 10.1007/s12603-018-1139-9. - DOI - PubMed
-
- Bhasin S., Travison T.G., Manini T.M., Patel S., Pencina K.M., Fielding R.A., Magaziner J.M., Newman A.B., Kiel D.P., Cooper C., et al. Sarcopenia Definition: The Position Statements of the Sarcopenia Definition and Outcomes Consortium. J. Am. Geriatr. Soc. 2020;68:1410–1418. doi: 10.1111/jgs.16372. - DOI - PMC - PubMed
-
- Ackermans L.L.G.C., Rabou J., Basrai M., Schweinlin A., Bischoff S.C., Cussenot O., Cancel-Tassin G., Renken R.J., Gómez E., Sánchez-González P., et al. Screening, Diagnosis and Monitoring of Sarcopenia: When to Use Which Tool? Clin. Nutr. ESPEN. 2022;48:36–44. doi: 10.1016/j.clnesp.2022.01.027. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
