

Pharmacological Therapy in Inflammatory Bowel Diseases: A Narrative Review of the Past 90 Years
- PMID: 37765080
- PMCID: PMC10537095
- DOI: 10.3390/ph16091272
Pharmacological Therapy in Inflammatory Bowel Diseases: A Narrative Review of the Past 90 Years
Abstract
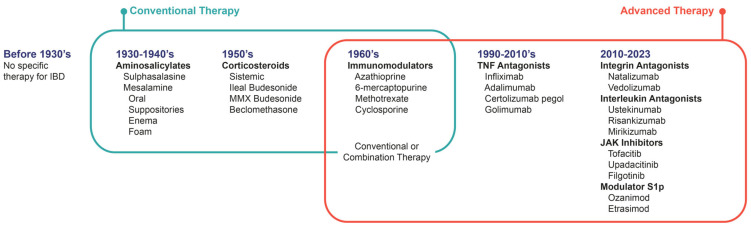
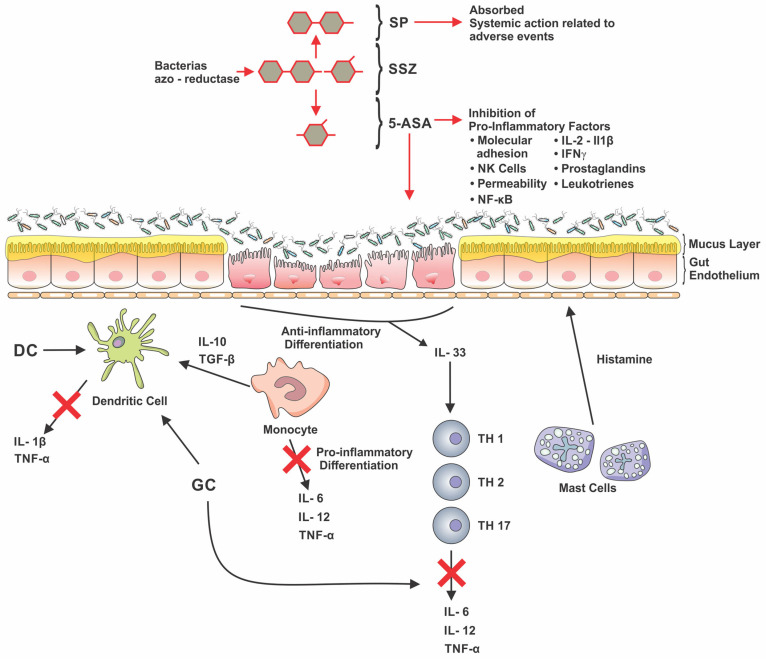
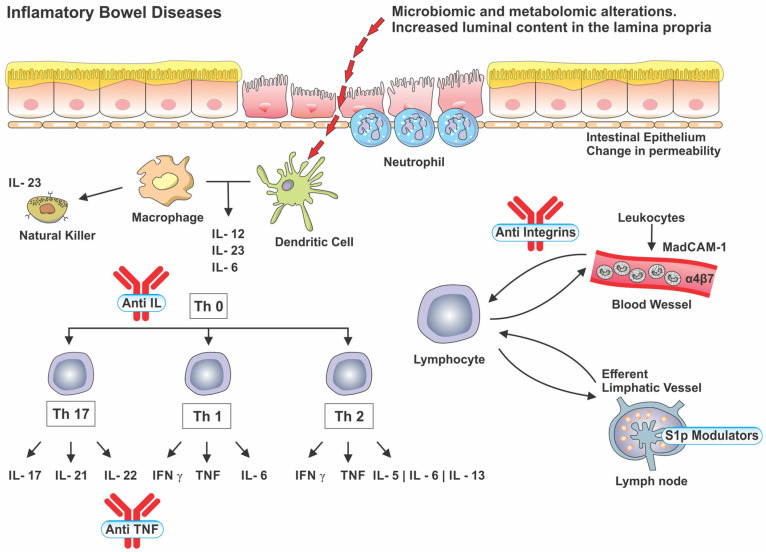
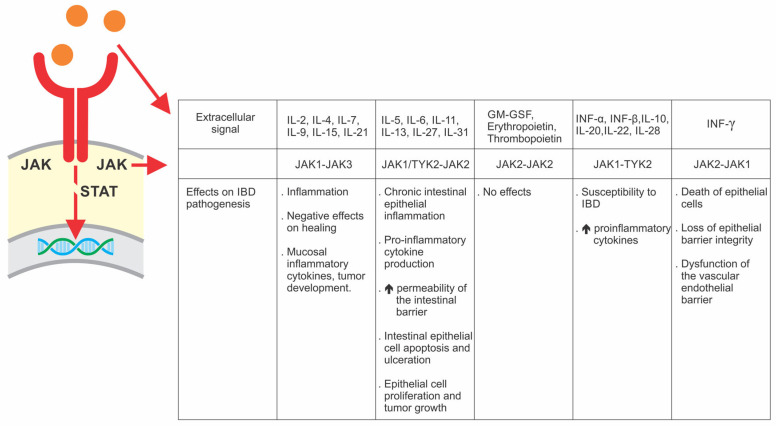
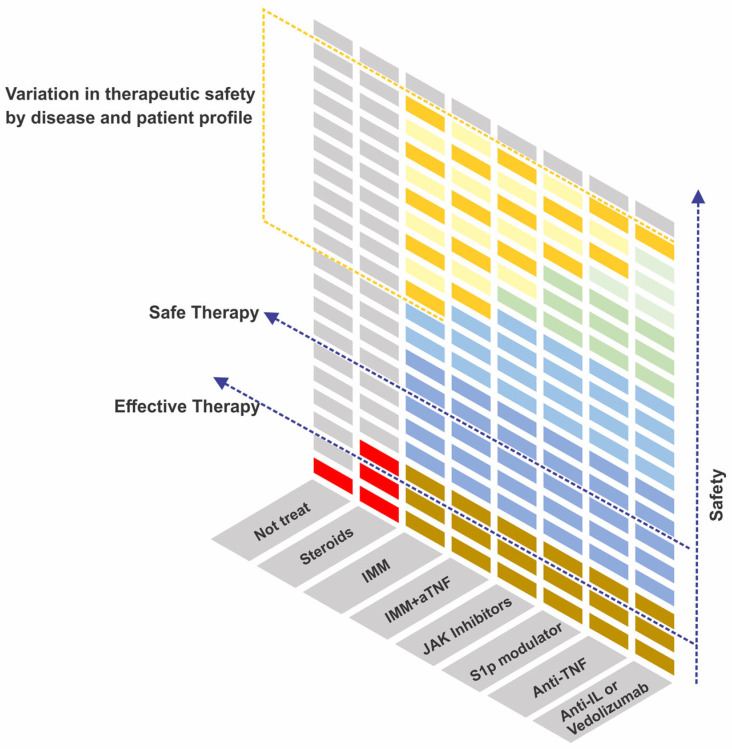
Inflammatory Bowel Diseases had their first peak in incidence in countries in North America, Europe, and Oceania and are currently experiencing a new acceleration in incidence, especially in Latin America and Asia. Despite technological advances, 90 years after the development of the first molecule for the treatment of IBD, we still do not have drugs that promote disease remission in a generalized way. We carried out a narrative review on therapeutic advances in the treatment of IBD, the mechanisms of action, and the challenges facing the therapeutic goals in the treatment of IBD. Salicylates are still used in the treatment of Ulcerative Colitis. Corticosteroids have an indication restricted to the period of therapeutic induction due to frequent adverse events, while technologies with less systemic action have been developed. Most immunomodulators showed a late onset of action, requiring a differentiated initial strategy to control the disease. New therapeutic perspectives emerged with biological therapy, initially with anti-TNF, followed by anti-integrins and anti-interleukins. Despite the different mechanisms of action, there are similarities between the general rates of effectiveness. These similar results were also evidenced in JAK inhibitors and S1p modulators, the last therapeutic classes approved for the treatment of IBD.
Keywords: 5-ASA; Crohn’s disease; JAK; biological therapy; corticosteroid; immunomodulator; s1P; ulcerative colitis.
Conflict of interest statement
MI reports personal fees from AbbVie, Ferring, Nestle, Janssen, Takeda and Pfizer. F Magro severd as speaker for: Abbvie, Arena, Biogen, Bristol-Myers Squibb, Falk, Ferring, Hospira, Janssen, Laboratórios Vitoria, Pfizer, Lilly, Merck Sharp & Dohme, Sandoz, Takeda, UCB, Vifor.
Figures
References
-
- Celebi Sozener Z., Ozdel Ozturk B., Cerci P., Turk M., Gorgulu Akin B., Akdis M., Altiner S., Ozbey U., Ogulur I., Mitamura Y., et al. Epithelial Barrier Hypothesis: Effect of the External Exposome on the Microbiome and Epithelial Barriers in Allergic Disease. Allergy. 2022;77:1418–1449. doi: 10.1111/all.15240. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
