

Cutaneous Cell Therapy Manufacturing Timeframe Rationalization: Allogeneic Off-the-Freezer Fibroblasts for Dermo-Epidermal Combined Preparations (DE-FE002-SK2) in Burn Care
- PMID: 37765300
- PMCID: PMC10536166
- DOI: 10.3390/pharmaceutics15092334
Cutaneous Cell Therapy Manufacturing Timeframe Rationalization: Allogeneic Off-the-Freezer Fibroblasts for Dermo-Epidermal Combined Preparations (DE-FE002-SK2) in Burn Care
Abstract
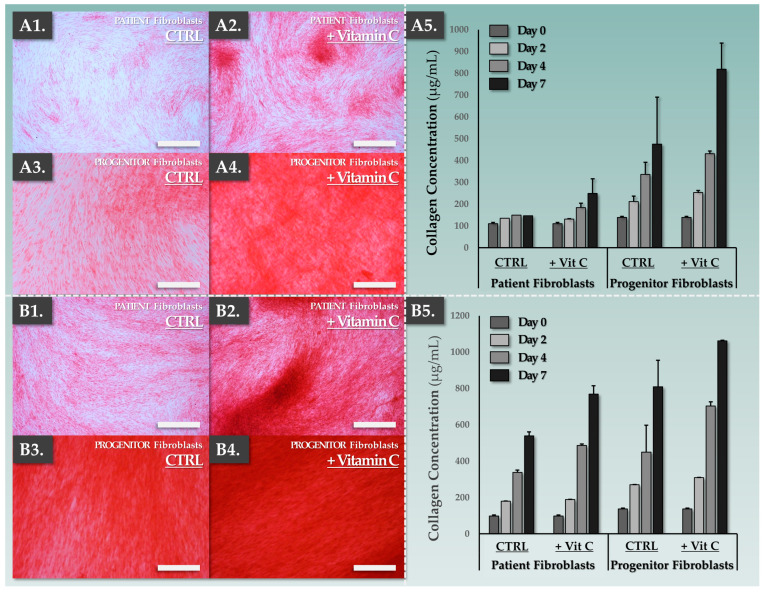
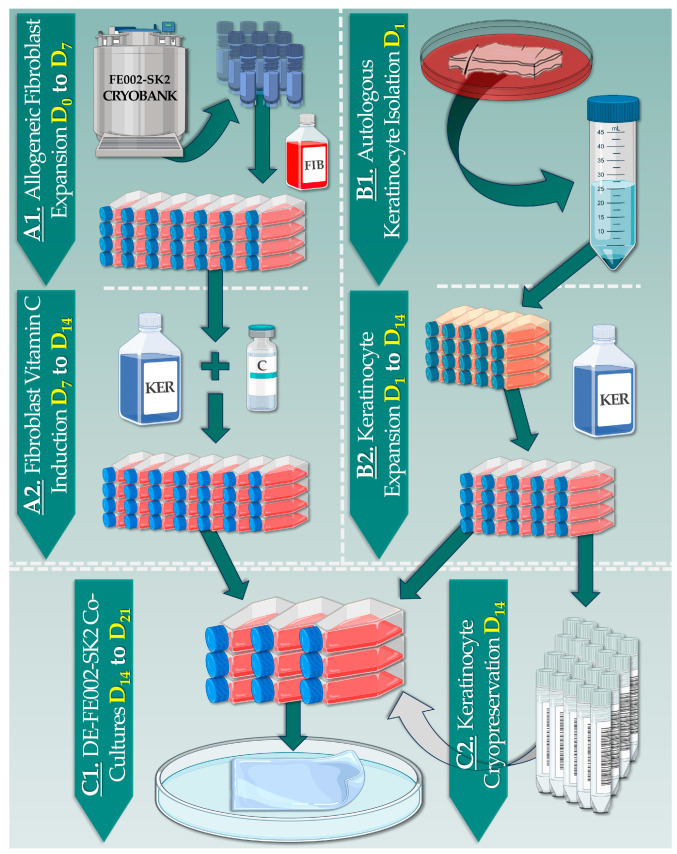
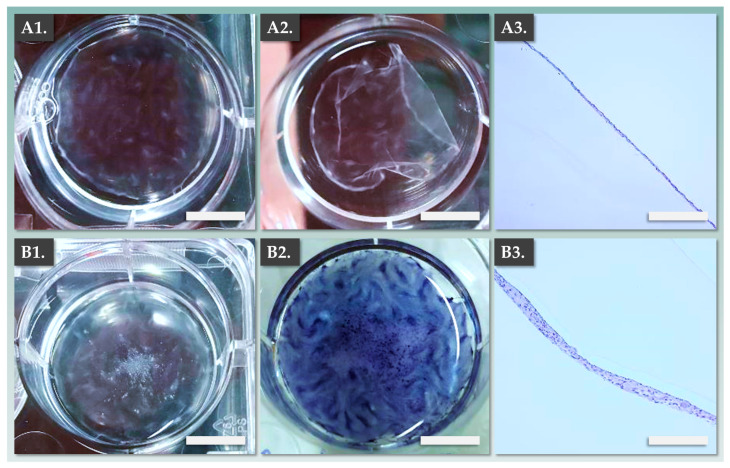
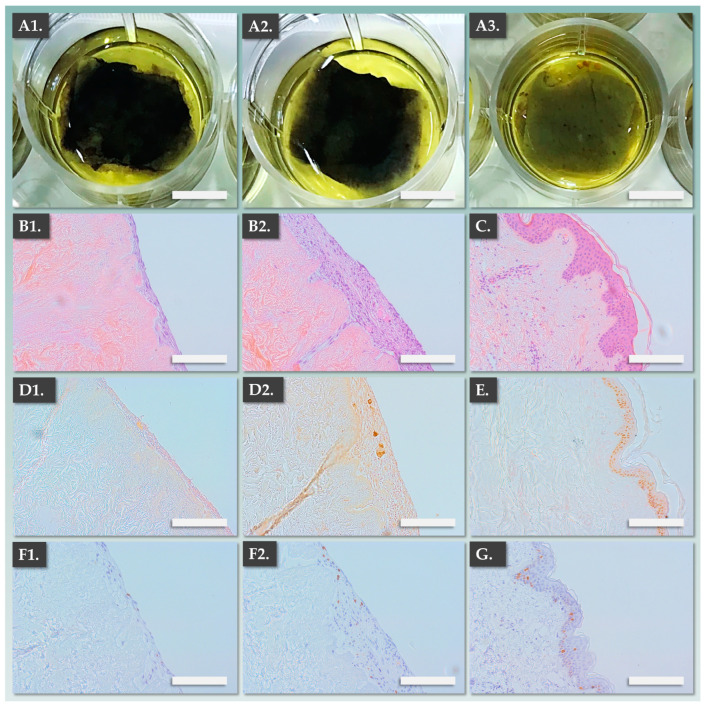
Autologous cell therapy manufacturing timeframes constitute bottlenecks in clinical management pathways of severe burn patients. While effective temporary wound coverings exist for high-TBSA burns, any means to shorten the time-to-treatment with cytotherapeutic skin grafts could provide substantial therapeutic benefits. This study aimed to establish proofs-of-concept for a novel combinational cytotherapeutic construct (autologous/allogeneic DE-FE002-SK2 full dermo-epidermal graft) designed for significant cutaneous cell therapy manufacturing timeframe rationalization. Process development was based on several decades (four for autologous protocols, three for allogeneic protocols) of in-house clinical experience in cutaneous cytotherapies. Clinical grade dermal progenitor fibroblasts (standardized FE002-SK2 cell source) were used as off-the-freezer substrates in novel autologous/allogeneic dermo-epidermal bilayer sheets. Under vitamin C stimulation, FE002-SK2 primary progenitor fibroblasts rapidly produced robust allogeneic dermal templates, allowing patient keratinocyte attachment in co-culture. Notably, FE002-SK2 primary progenitor fibroblasts significantly outperformed patient fibroblasts for collagen deposition. An ex vivo de-epidermalized dermis model was used to demonstrate the efficient DE-FE002-SK2 construct bio-adhesion properties. Importantly, the presented DE-FE002-SK2 manufacturing process decreased clinical lot production timeframes from 6-8 weeks (standard autologous combined cytotherapies) to 2-3 weeks. Overall, these findings bear the potential to significantly optimize burn patient clinical pathways (for rapid wound closure and enhanced tissue healing quality) by combining extensively clinically proven cutaneous cell-based technologies.
Keywords: FE002 dermal progenitor fibroblasts; autologous keratinocytes; burn center; cutaneous cell therapy; dermal template; dermo-epidermal grafts; early coverage solutions; manufacturing optimization; severe burns; standardized skin grafts.
Conflict of interest statement
Author A.L. was employed by TEC-PHARMA SA (Bercher, Switzerland) and by LAM Biotechnologies SA (Epalinges, Switzerland) during the course of the study, within the scope of an industrial thesis. The remaining authors declare no conflict of interest.
Figures

Similar articles
-
Bicomponent Cutaneous Cell Therapy for Early Burn Care: Manufacturing Homogeneity and Epidermis-Structuring Functions of Clinical Grade FE002-SK2 Allogeneic Dermal Progenitor Fibroblasts.Pharmaceutics. 2025 May 24;17(6):692. doi: 10.3390/pharmaceutics17060692. Pharmaceutics. 2025. PMID: 40574004 Free PMC article.
-
Autologous and Allogeneic Cytotherapies for Large Knee (Osteo)Chondral Defects: Manufacturing Process Benchmarking and Parallel Functional Qualification.Pharmaceutics. 2023 Sep 16;15(9):2333. doi: 10.3390/pharmaceutics15092333. Pharmaceutics. 2023. PMID: 37765301 Free PMC article.
-
Bio-Enhanced Neoligaments Graft Bearing FE002 Primary Progenitor Tenocytes: Allogeneic Tissue Engineering & Surgical Proofs-of-Concept for Hand Ligament Regenerative Medicine.Pharmaceutics. 2023 Jul 3;15(7):1873. doi: 10.3390/pharmaceutics15071873. Pharmaceutics. 2023. PMID: 37514060 Free PMC article.
-
Tissue-engineered skin. Current status in wound healing.Am J Clin Dermatol. 2001;2(5):305-13. doi: 10.2165/00128071-200102050-00005. Am J Clin Dermatol. 2001. PMID: 11721649 Review.
-
Understanding experimental biology of skin equivalent: from laboratory to clinical use in patients with burns and chronic wounds.Am J Surg. 2004 May;187(5A):29S-33S. doi: 10.1016/S0002-9610(03)00301-5. Am J Surg. 2004. PMID: 15147989 Review.
Cited by
-
Optimization and Standardization of Stable De-Epidermized Dermis (DED) Models for Functional Evaluation of Cutaneous Cell Therapies.Bioengineering (Basel). 2024 Dec 20;11(12):1297. doi: 10.3390/bioengineering11121297. Bioengineering (Basel). 2024. PMID: 39768115 Free PMC article.
-
Bicomponent Cutaneous Cell Therapy for Early Burn Care: Manufacturing Homogeneity and Epidermis-Structuring Functions of Clinical Grade FE002-SK2 Allogeneic Dermal Progenitor Fibroblasts.Pharmaceutics. 2025 May 24;17(6):692. doi: 10.3390/pharmaceutics17060692. Pharmaceutics. 2025. PMID: 40574004 Free PMC article.
-
A novel method for the establishment of autologous skin cell suspensions: characterisation of cellular sub-populations, epidermal stem cell content and wound response-enhancing biological properties.Front Bioeng Biotechnol. 2024 Apr 5;12:1386896. doi: 10.3389/fbioe.2024.1386896. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38646012 Free PMC article.
References
-
- Schlottmann F., Bucan V., Vogt P.M., Krezdorn N. A short history of skin grafting in burns: From the gold standard of autologous skin grafting to the possibilities of allogeneic skin grafting with immunomodulatory approaches. Medicina. 2021;57:225. doi: 10.3390/medicina57030225. - DOI - PMC - PubMed
-
- Chemali M., Laurent A., Scaletta C., Waselle L., Simon J.-P., Michetti M., Brunet J.-F., Flahaut M., Hirt-Burri N., Raffoul W., et al. Burn center organization and cellular therapy integration: Managing risks and costs. J. Burn Care Res. 2021;42:911–924. doi: 10.1093/jbcr/irab080. - DOI - PMC - PubMed
-
- Münzberg M., Ziegler B., Fischer S., Wölfl C.G., Grützner P.A., Kremer T., Kneser U., Hirche C. In view of standardization: Comparison and analysis of initial management of severely burned patients in Germany, Austria and Switzerland. Burns. 2015;41:33–38. doi: 10.1016/j.burns.2014.08.021. - DOI - PubMed
LinkOut - more resources
Full Text Sources
