

Autologous and Allogeneic Cytotherapies for Large Knee (Osteo)Chondral Defects: Manufacturing Process Benchmarking and Parallel Functional Qualification
- PMID: 37765301
- PMCID: PMC10536774
- DOI: 10.3390/pharmaceutics15092333
Autologous and Allogeneic Cytotherapies for Large Knee (Osteo)Chondral Defects: Manufacturing Process Benchmarking and Parallel Functional Qualification
Abstract
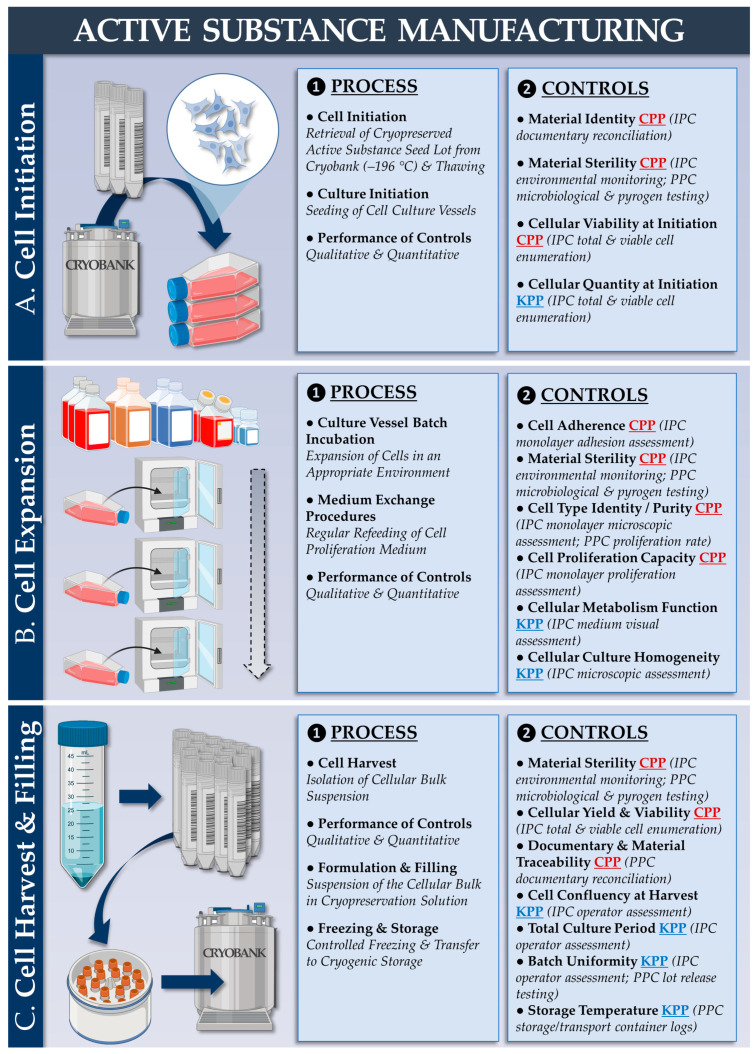
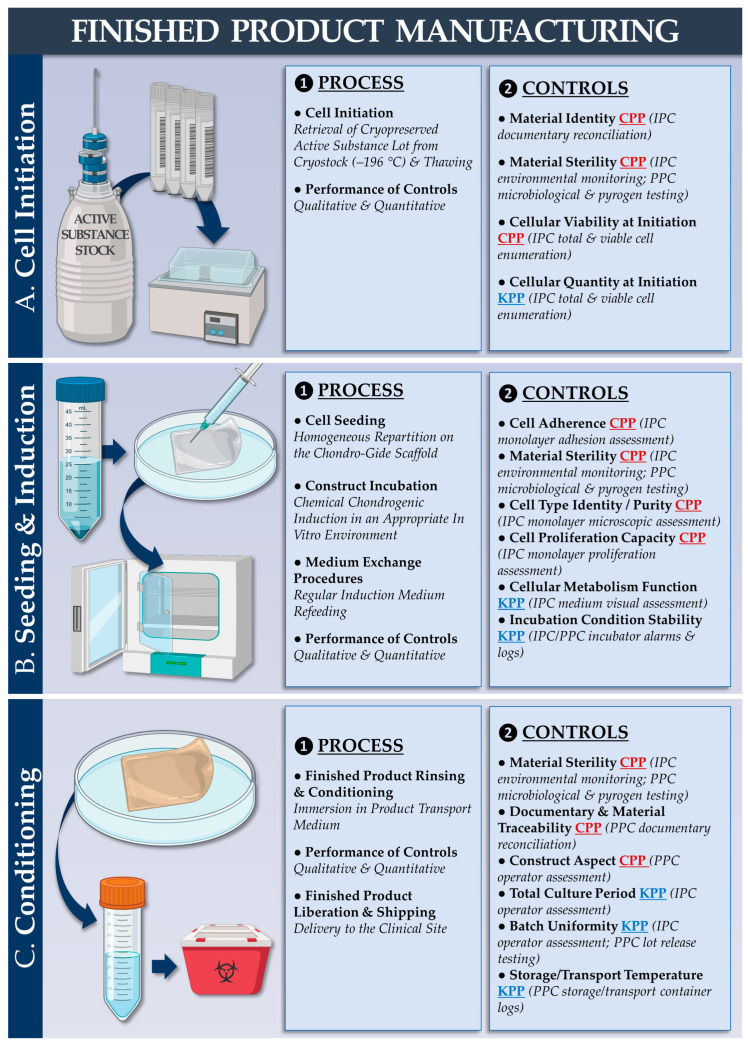
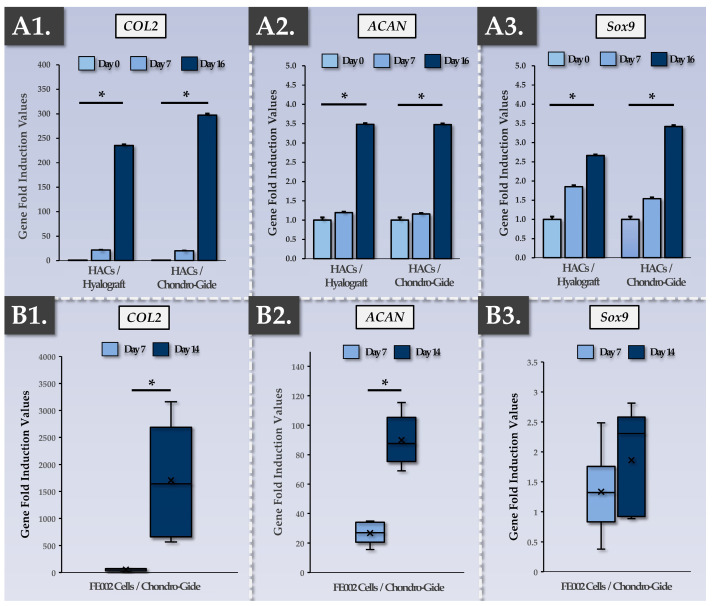
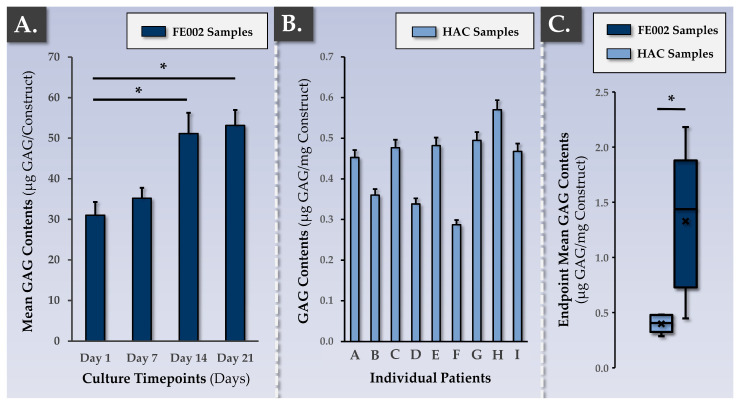
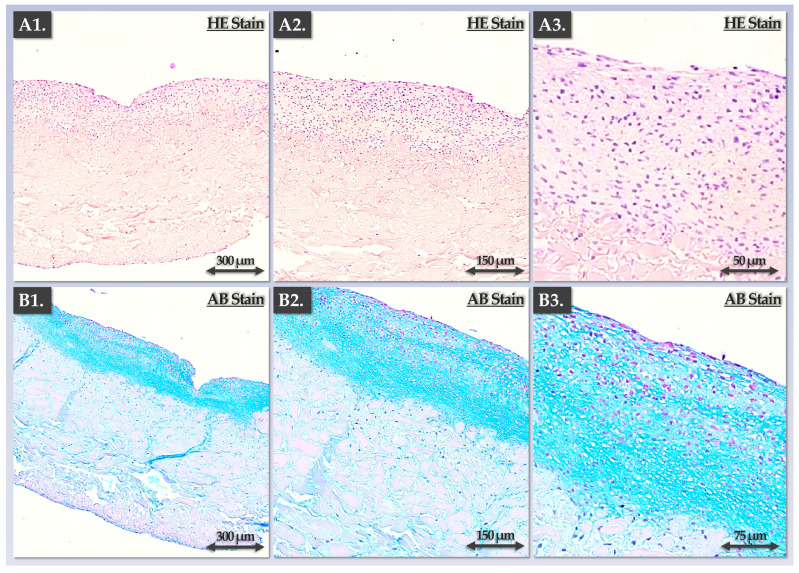
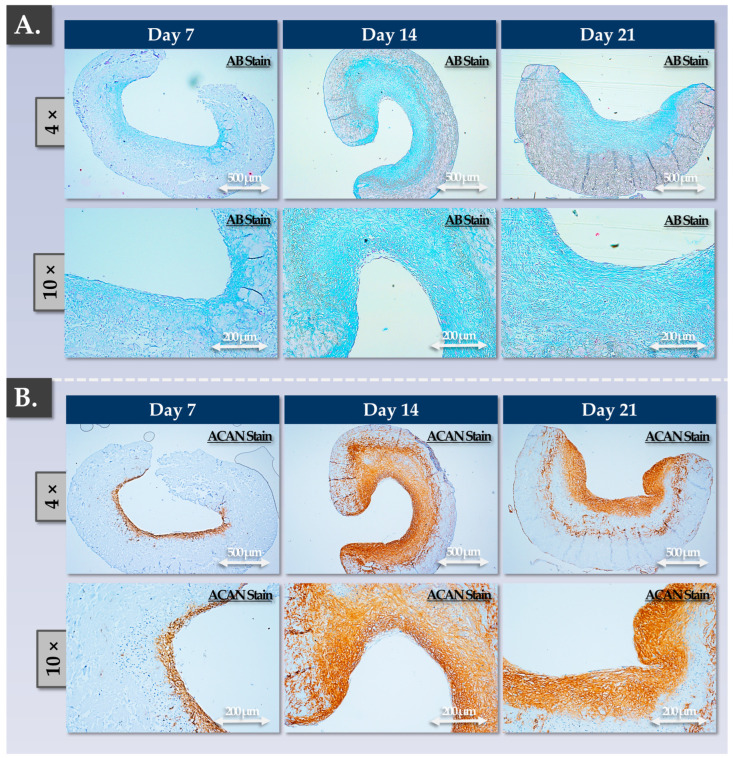
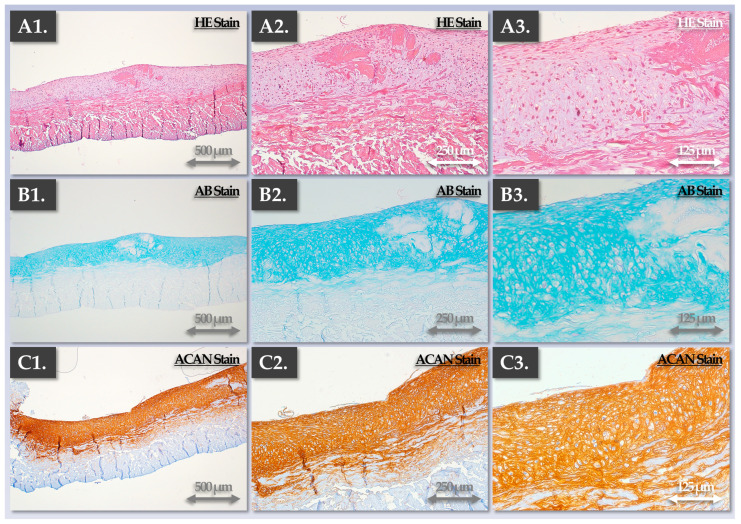
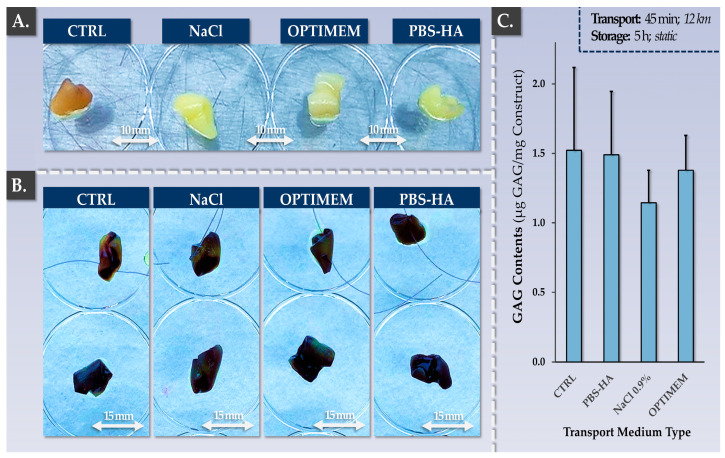
Cytotherapies are often necessary for the management of symptomatic large knee (osteo)-chondral defects. While autologous chondrocyte implantation (ACI) has been clinically used for 30 years, allogeneic cells (clinical-grade FE002 primary chondroprogenitors) have been investigated in translational settings (Swiss progenitor cell transplantation program). The aim of this study was to comparatively assess autologous and allogeneic approaches (quality, safety, functional attributes) to cell-based knee chondrotherapies developed for clinical use. Protocol benchmarking from a manufacturing process and control viewpoint enabled us to highlight the respective advantages and risks. Safety data (telomerase and soft agarose colony formation assays, high passage cell senescence) and risk analyses were reported for the allogeneic FE002 cellular active substance in preparation for an autologous to allogeneic clinical protocol transposition. Validation results on autologous bioengineered grafts (autologous chondrocyte-bearing Chondro-Gide scaffolds) confirmed significant chondrogenic induction (COL2 and ACAN upregulation, extracellular matrix synthesis) after 2 weeks of co-culture. Allogeneic grafts (bearing FE002 primary chondroprogenitors) displayed comparable endpoint quality and functionality attributes. Parameters of translational relevance (transport medium, finished product suturability) were validated for the allogeneic protocol. Notably, the process-based benchmarking of both approaches highlighted the key advantages of allogeneic FE002 cell-bearing grafts (reduced cellular variability, enhanced process standardization, rationalized logistical and clinical pathways). Overall, this study built on our robust knowledge and local experience with ACI (long-term safety and efficacy), setting an appropriate standard for further clinical investigations into allogeneic progenitor cell-based orthopedic protocols.
Keywords: FE002 primary chondroprogenitors; allogeneic cytotherapies; autologous chondrocyte implantation; cartilage defect; cell therapy; chondrogenesis; manufacturing process; standardized transplant product; tissue engineering; translational research.
Conflict of interest statement
Authors A.J., C.P. and A.L. were employed by LAM Biotechnologies SA (Epalinges, Switzerland) during the production of this work. The remaining authors declare no conflicts of interest.
Figures
References
-
- Niemeyer P., Hanus M., Belickas J., László T., Gudas R., Fiodorovas M., Cebatorius A., Pastucha M., Hoza P., Magos K., et al. Treatment of large cartilage defects in the knee by hydrogel-based autologous chondrocyte implantation: Two-year results of a prospective, multicenter, single-arm phase III trial. Cartilage. 2022;13:19476035221085146. doi: 10.1177/19476035221085146. - DOI - PMC - PubMed
-
- Saris D.B., Vanlauwe J., Victor J., Almqvist K.F., Verdonk R., Bellemans J., Luyten F.P., TIG/ACT/01/2000&EXT Study Group Treatment of symptomatic cartilage defects of the knee: Characterized chondrocyte implantation results in better clinical outcome at 36 months in a randomized trial compared to microfracture. Am. J. Sports Med. 2009;37:10S–19S. doi: 10.1177/0363546509350694. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
