

General prognostic models may neglect vulnerable subgroups in ANCA-associated vasculitis
- PMID: 37768548
- PMCID: PMC10638135
- DOI: 10.1007/s40620-023-01726-5
General prognostic models may neglect vulnerable subgroups in ANCA-associated vasculitis
Abstract
Background: ANCA-associated vasculitis is an organ and life-threatening disease with the highest incidence in elderly patients. However, few studies have focussed on characteristics and treatment outcomes in a direct comparison of elderly and younger patients.
Methods: In a retrospective, single-centre, renal biopsy-cohort, patients were dichotomized by age ≥ 65 years to analyse baseline clinical, histological, laboratory and immunological characteristics and outcome differences in elderly and younger patients as regard to mortality, renal recovery from dialysis and eGFR after two years.
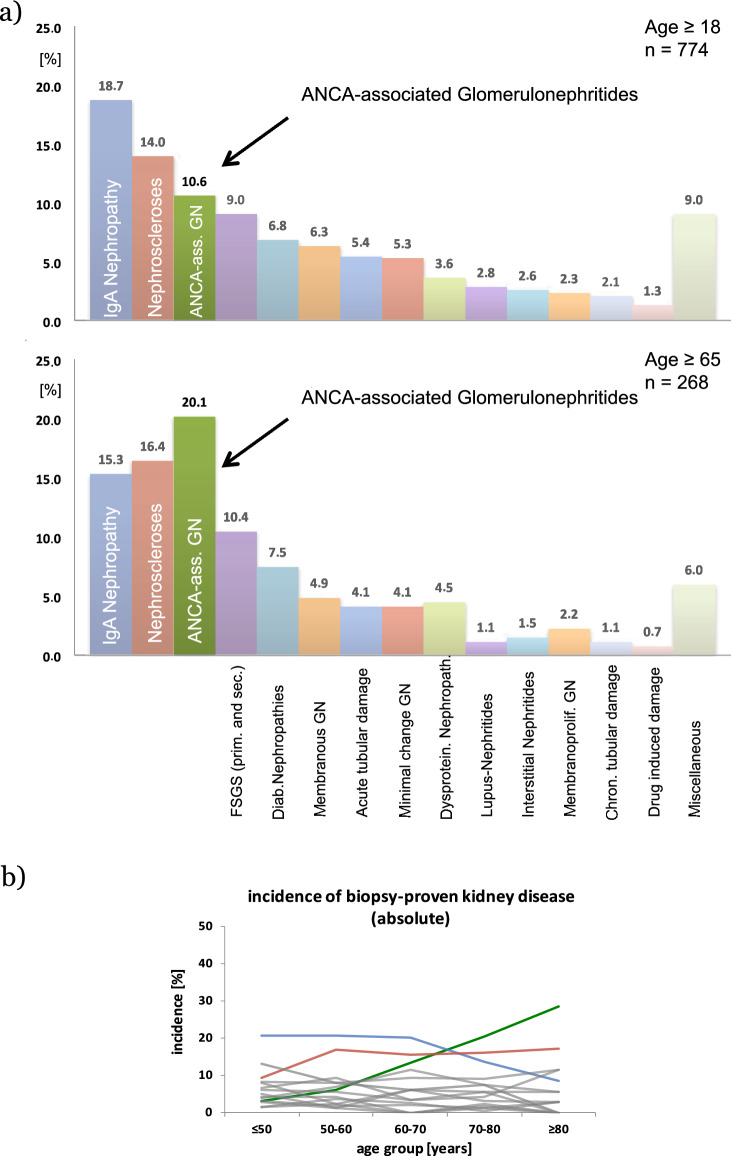
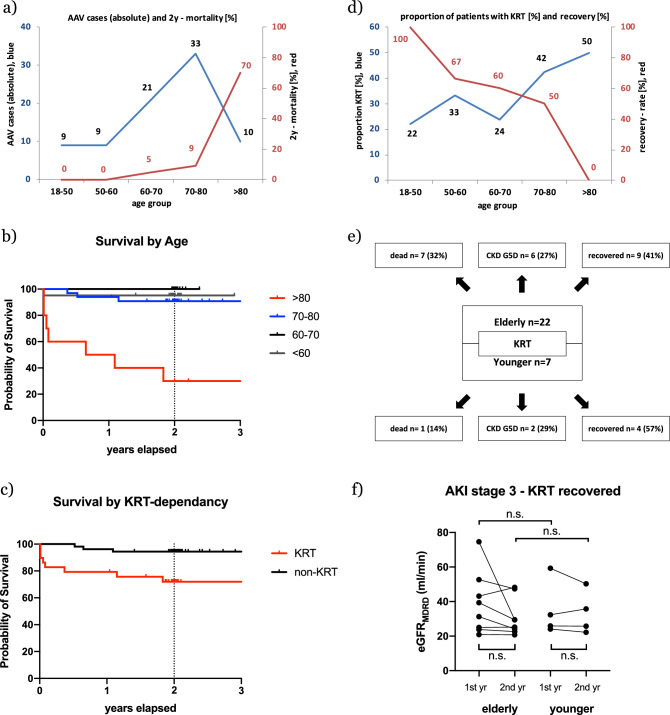
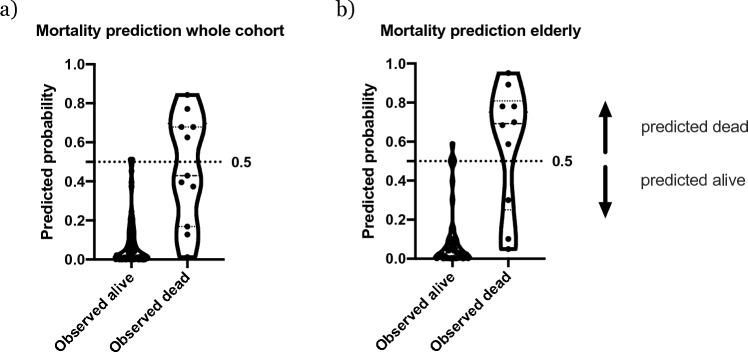
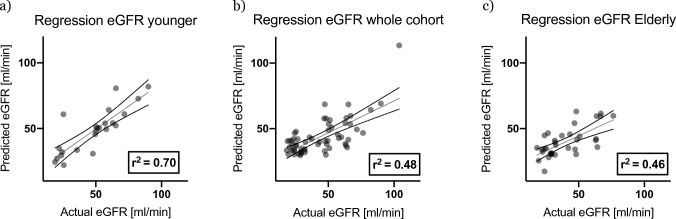
Results: In the biopsy registry, n = 774 patients were identified, of whom 268 were ≥ 65 years old. Among them, ANCA-associated vasculitis was the most prevalent kidney disease (n = 54 ≈ 20%). After a follow-up of 2 years, overall mortality was 13.4%, with 19% and 4% in patients ≥ and < 65 years of age, respectively. While 41% of elderly and 25% of younger patients were dialysis-dependent at the time of biopsy, renal recovery was achieved in 41% and 57% of patients, respectively. The accuracy of prediction differed significantly between the whole cohort and elderly patients as regard to mortality (sensitivity 46% vs. 90%, respectively) and between younger and elderly patients as regard to eGFR (r2 = 0.7 vs. 0.46, respectively). Age-group-wise analysis revealed patients above 80 years of age to have particularly dismal renal outcome and survival.
Conclusion: In our cohort, ANCA-associated vasculitis is the single most frequent histopathological diagnosis among the elderly patients in our cohort. Elderly and younger patients have comparable chances of recovering from dialysis-dependent renal failure, with comparable residual independent kidney function after two years. This study suggests (1) relevant predictors differ between age groups and hence (2) models involving all patients with ANCA-associated vasculitis neglect important features of vulnerable subgroups, i.e., patients above 80 years old.
Keywords: ANCA-associated vasculitis; Elderly; Mortality; Outcome; Renal recovery; Renal replacement therapy; Survival.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
