

Fibroblasts in heart scar tissue directly regulate cardiac excitability and arrhythmogenesis
- PMID: 37769108
- PMCID: PMC10768850
- DOI: 10.1126/science.adh9925
Fibroblasts in heart scar tissue directly regulate cardiac excitability and arrhythmogenesis
Abstract
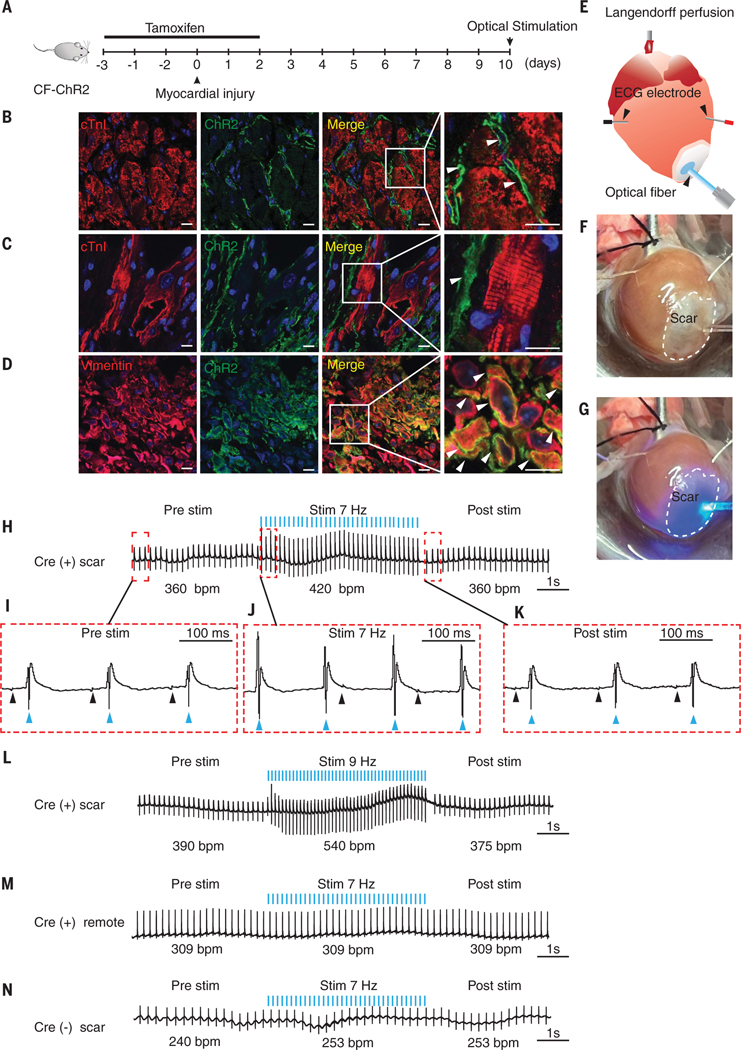
After heart injury, dead heart muscle is replaced by scar tissue. Fibroblasts can electrically couple with myocytes, and changes in fibroblast membrane potential can lead to myocyte excitability, which suggests that fibroblast-myocyte coupling in scar tissue may be responsible for arrhythmogenesis. However, the physiologic relevance of electrical coupling of myocytes and fibroblasts and its impact on cardiac excitability in vivo have never been demonstrated. We genetically engineered a mouse that expresses the optogenetic cationic channel ChR2 (H134R) exclusively in cardiac fibroblasts. After myocardial infarction, optical stimulation of scar tissue elicited organ-wide cardiac excitation and induced arrhythmias in these animals. Complementing computational modeling with experimental approaches, we showed that gap junctional and ephaptic coupling, in a synergistic yet functionally redundant manner, excited myocytes coupled to fibroblasts.
Conflict of interest statement
Figures



Comment in
-
Depolarization of fibroblasts in scar tissue drives cardiac excitation.Nat Rev Cardiol. 2023 Dec;20(12):795. doi: 10.1038/s41569-023-00948-1. Nat Rev Cardiol. 2023. PMID: 37848629 No abstract available.
-
Fibroblasts, myofibroblasts and cardiac arrhythmias.J Cardiovasc Aging. 2023 Oct;3(4):43. doi: 10.20517/jca.2023.37. Epub 2023 Oct 25. J Cardiovasc Aging. 2023. PMID: 38235057 Free PMC article. No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
