

IVIg Use Associated with Ten-Fold Reduction of Serious Infections in Multiple Myeloma Patients Treated with Anti-BCMA Bispecific Antibodies
- PMID: 37769148
- PMCID: PMC10618720
- DOI: 10.1158/2643-3230.BCD-23-0049
IVIg Use Associated with Ten-Fold Reduction of Serious Infections in Multiple Myeloma Patients Treated with Anti-BCMA Bispecific Antibodies
Abstract
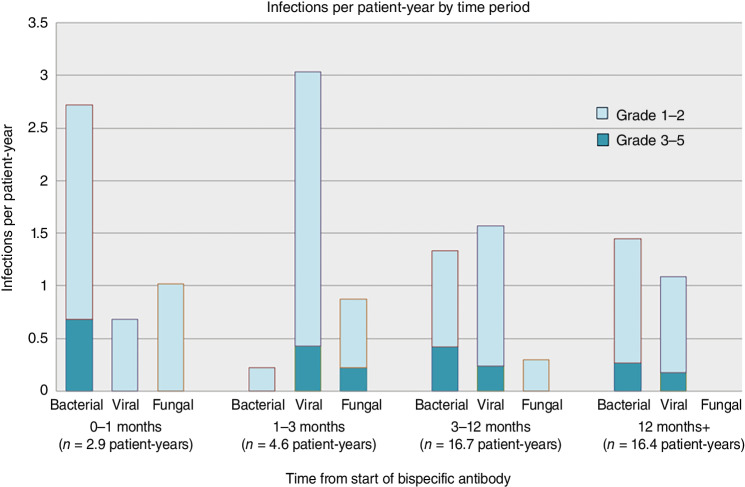
BCMA-targeted bispecific antibodies (BiAb) are efficacious in relapsed/refractory multiple myeloma; however, serious infections have emerged as important toxicities. In this retrospective study, we characterized all infections and their risk factors, and evaluated the impact of infection prophylaxis in patients treated with BCMA-targeted BiAbs. Among 37 patients, 15 (41%) experienced a grade 3-5 infection, with two infection-related deaths during deep remissions. Most (84%) infections occurred during disease remissions. The cumulative probability of grade 3-5 infection increased over time with no plateau. Among responders (n = 26), profound hypogammaglobulinemia occurred in 100% and continued throughout the entire duration of treatment. During periods when patients were receiving intravenous immunoglobulin (IVIg), the rate of grade 3-5 infections was 90% lower than during observation (incidence rate ratio, 0.10; 95% confidence interval, 0.01-0.80; P = 0.0307). No other risk factors for infection were identified. This study demonstrates that profound hypogammaglobulinemia is universal with BCMA-targeted BiAbs, with intravenous immunoglobulin potentially abrogating most of the infection risk.
Significance: To the best of our knowledge, this is the first study to comprehensively analyze risk factors and mitigation strategies to prevent infections in myeloma patients receiving anti-BCMA bispecific antibodies. Profound and prolonged hypogammaglobulinemia was universal among responders, while immunoglobulin replacement was associated with 90% lower rates of grade 3-5 infections. See related commentary by Garfall and Stadtmauer, p. 427 . This article is featured in Selected Articles from This Issue, p. 419.
©2023 American Association for Cancer Research.
Figures



Comment in
-
Understanding Infection Risk with Anti-BCMA Bispecific Antibodies.Blood Cancer Discov. 2023 Nov 1;4(6):427-429. doi: 10.1158/2643-3230.BCD-23-0157. Blood Cancer Discov. 2023. PMID: 37769160 Free PMC article.
References
-
- Raje N, Bahlis NJ, Costello C, Dholaria B, Solh M, Levy MY, et al. . Elranatamab, a BCMA targeted T-cell engaging bispecific antibody, induces durable clinical and molecular responses for patients with relapsed or refractory multiple myeloma. Blood 2022;140( Suppl 1):388–90. - PubMed
-
- Wong SW, Bar N, Paris L, Hofmeister CC, Hansson M, Santoro A, et al. . Alnuctamab (ALNUC; BMS-986349; CC-93269), a B-cell maturation antigen (BCMA) x CD3 T-cell engager (TCE), in patients (pts) with relapsed/refractory multiple myeloma (RRMM): results from a phase 1 first-in-human clinical study. Blood 2022;140( Suppl 1):400–2.
-
- Bumma N, Richter J, Brayer J, Zonder JA, Dhodapkar M, Shah MR, et al. . Updated safety and efficacy of REGN5458, a BCMAxCD3 bispecific antibody, treatment for relapsed/refractory multiple myeloma: a phase 1/2 first-in-human study. Blood 2022;140( Suppl 1):10140–1.
