

Perinatal Outcomes Associated With Management of Stage 1 Hypertension
- PMID: 37769314
- PMCID: PMC10840706
- DOI: 10.1097/AOG.0000000000005410
Perinatal Outcomes Associated With Management of Stage 1 Hypertension
Abstract
Objective: To evaluate the association between maternal blood pressure (BP) below 130/80 mm Hg compared with 130-139/80-89 mm Hg and pregnancy outcomes.
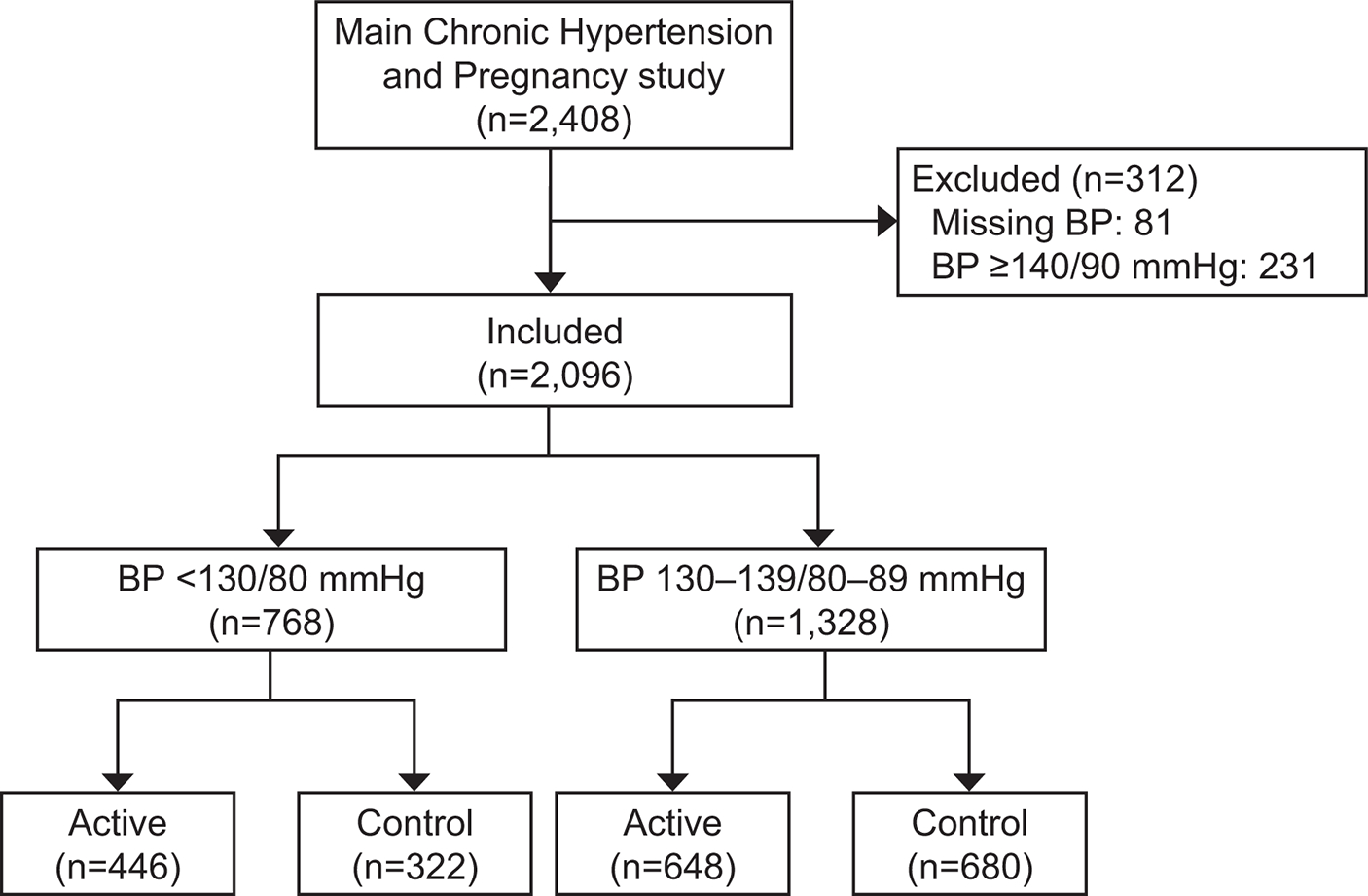
Methods: We conducted a planned secondary analysis of CHAP (Chronic Hypertension and Pregnancy), an open label, multicenter, randomized controlled trial. Participants with mean BP below 140/90 mm Hg were grouped as below 130/80 mm Hg compared with 130-139/80-89 mm Hg by averaging postrandomization clinic BP throughout pregnancy. The primary composite outcome was preeclampsia with severe features, indicated preterm birth before 35 weeks of gestation, placental abruption, or fetal or neonatal death. The secondary outcome was small for gestational age (SGA).
Results: Of 2,408 patients in CHAP, 2,096 met study criteria; 1,328 had mean BP 130-139/80-89 mm Hg and 768 had mean BP below 130/80 mm Hg. Participants with mean BP below 130/80 mm Hg were more likely to be older, on antihypertensive medication, in the active treatment arm, and to have lower BP at enrollment. Mean clinic BP below 130/80 mm Hg was associated with lower frequency of the primary outcome (16.0% vs 35.8%, adjusted relative risk 0.45; 95% CI 0.38-0.54) as well as lower risk of severe preeclampsia and indicated birth before 35 weeks of gestation. There was no association with SGA.
Conclusion: In pregnant patients with mild chronic hypertension, mean BP below 130/80 mm Hg was associated with improved pregnancy outcomes without increased risk of SGA.
Clinical trial registration: ClinicalTrials.gov , NCT02299414.
Copyright © 2023 by the American College of Obstetricians and Gynecologists. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure Alan T.N. Tita reported money was paid to his institution by Pfizer for his efforts on this study. Torri D. Metz disclosed money was paid to her from UpToDate for two topics on trial of labor after cesarean, and money was paid to her institution from Gestvision as a site PI for a preeclampsia point-of-care test; her institution received money to conduct the study (ended August 2020). She has been a site PI for Pfizer on a phase III RSV vaccine trial, and her institution received money to conduct the study. She has also been a member of the Pfizer medical advisory board (1/15/21) and site PI for a COVID-19 vaccination trial in pregnancy. She has served on the SMFM Board of Directors. Lorraine Dugoff reports money was paid to her institution from Laboratory Holdings, Inc. and Natera, Inc. Brenna L. Hughes reports receiving payment from UpToDate. Mary E. Norton reports receiving payment from the American Board of Obstetrics and Gynecology and Luna Genetics. Daniel Skupski disclosed he is a consultant for Cooper Surgical, Inc, and has received payment from Organon. Namasivayam Ambalayanan reports receiving payment from Resbiotic/AlveolusBio and Shire/Oak Hill Bio. The other authors did not report any potential conflicts of interest.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
