

Polygenic risk scores of lithium response and treatment resistance in major depressive disorder
- PMID: 37770441
- PMCID: PMC10539379
- DOI: 10.1038/s41398-023-02602-3
Polygenic risk scores of lithium response and treatment resistance in major depressive disorder
Abstract
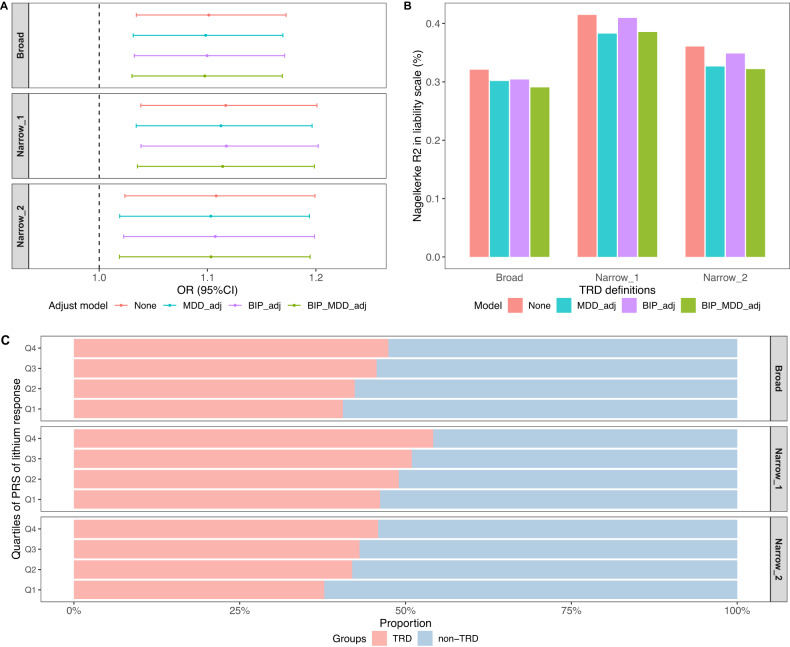
Treatment response and resistance in major depressive disorder (MDD) are suggested to be heritable. Due to significant challenges in defining treatment-related phenotypes, our understanding of their genetic bases is limited. This study aimed to derive a stringent definition of treatment resistance and to investigate the genetic overlap between treatment response and resistance in MDD. Using electronic medical records on the use of antidepressants and electroconvulsive therapy (ECT) from Swedish registers, we derived the phenotype of treatment-resistant depression (TRD) and non-TRD within ~4500 individuals with MDD in three Swedish cohorts. Considering antidepressants and lithium are first-line treatment and augmentation used for MDD, respectively, we generated polygenic risk scores (PRS) of antidepressants and lithium response for individuals with MDD and evaluated their associations with treatment resistance by comparing TRD with non-TRD. Among 1778 ECT-treated MDD cases, nearly all (94%) used antidepressants before their first ECT and the vast majority had at least one (84%) or two (61%) antidepressants of adequate duration, suggesting these MDD cases receiving ECT were resistant to antidepressants. We did not observe a significant difference in the mean PRS of antidepressant response between TRD and non-TRD; however, we found that TRD cases had a significantly higher PRS of lithium response compared to non-TRD cases (OR = 1.10-1.12 under various definitions). The results support the evidence of heritable components in treatment-related phenotypes and highlight the overall genetic profile of lithium-sensitivity in TRD. This finding further provides a genetic explanation for lithium efficacy in treating TRD.
© 2023. Springer Nature Limited.
Conflict of interest statement
PFS is a consultant and shareholder for Neumora Therarapeutics. ML declares that he has received lecture honoraria from Lundbeck Pharmaceutical and served as a consultant for AstraZeneca. CML sits on the SAB for Myriad Neuroscience. All other authors report no biomedical financial interests or potential conflicts of interest related to this work.
Figures
Update of
-
Investigating genetic overlap between antidepressant and lithium response and treatment resistance in major depressive disorder.Res Sq [Preprint]. 2023 Feb 20:rs.3.rs-2556941. doi: 10.21203/rs.3.rs-2556941/v1. Res Sq. 2023. Update in: Transl Psychiatry. 2023 Sep 28;13(1):301. doi: 10.1038/s41398-023-02602-3. PMID: 36865283 Free PMC article. Updated. Preprint.
Similar articles
-
Investigating genetic overlap between antidepressant and lithium response and treatment resistance in major depressive disorder.Res Sq [Preprint]. 2023 Feb 20:rs.3.rs-2556941. doi: 10.21203/rs.3.rs-2556941/v1. Res Sq. 2023. Update in: Transl Psychiatry. 2023 Sep 28;13(1):301. doi: 10.1038/s41398-023-02602-3. PMID: 36865283 Free PMC article. Updated. Preprint.
-
Polygenic dissection of treatment-resistant depression with proxy phenotypes in the UK Biobank.J Affect Disord. 2025 Jul 15;381:350-359. doi: 10.1016/j.jad.2025.04.012. Epub 2025 Apr 3. J Affect Disord. 2025. PMID: 40187433
-
Higher polygenic risk scores for schizophrenia may be suggestive of treatment non-response in major depressive disorder.Prog Neuropsychopharmacol Biol Psychiatry. 2021 Jun 8;108:110170. doi: 10.1016/j.pnpbp.2020.110170. Epub 2020 Nov 10. Prog Neuropsychopharmacol Biol Psychiatry. 2021. PMID: 33181205
-
Efficacy and Tolerability of Combination Treatments for Major Depression: Antidepressants plus Second-Generation Antipsychotics vs. Esketamine vs. Lithium.J Psychopharmacol. 2021 Aug;35(8):890-900. doi: 10.1177/02698811211013579. Epub 2021 Jul 9. J Psychopharmacol. 2021. PMID: 34238049 Free PMC article.
-
Electroconvulsive Therapy for Treatment-Resistant Depression: Dispelling the Stigma.J Psychosoc Nurs Ment Health Serv. 2023 Jun;61(6):11-17. doi: 10.3928/02793695-20230222-02. Epub 2023 Mar 5. J Psychosoc Nurs Ment Health Serv. 2023. PMID: 36853035 Review.
Cited by
-
Genome-wide association meta-analysis and rare copy number variant analysis of treatment-resistant depression.Mol Psychiatry. 2025 Jun 26. doi: 10.1038/s41380-025-03084-z. Online ahead of print. Mol Psychiatry. 2025. PMID: 40571737
References
-
- Ekman M, Granström O, Omérov S, Jacob J, Landén M. The societal cost of depression: evidence from 10,000 Swedish patients in psychiatric care. J Affect Disord. 2013;150:790–7. - PubMed
-
- Bleakley S. Review of the choice and use of antidepressant drugs. Prog Neurol Psychiatry. 2013;17:18–26.
-
- Haddad PM, Talbot PS, Anderson IM, McAllister-Williams RH. Managing inadequate antidepressant response in depressive illness. Br Med Bull. 2015;115:183–201. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
