

Garetosmab in fibrodysplasia ossificans progressiva: a randomized, double-blind, placebo-controlled phase 2 trial
- PMID: 37770652
- PMCID: PMC10579054
- DOI: 10.1038/s41591-023-02561-8
Garetosmab in fibrodysplasia ossificans progressiva: a randomized, double-blind, placebo-controlled phase 2 trial
Abstract
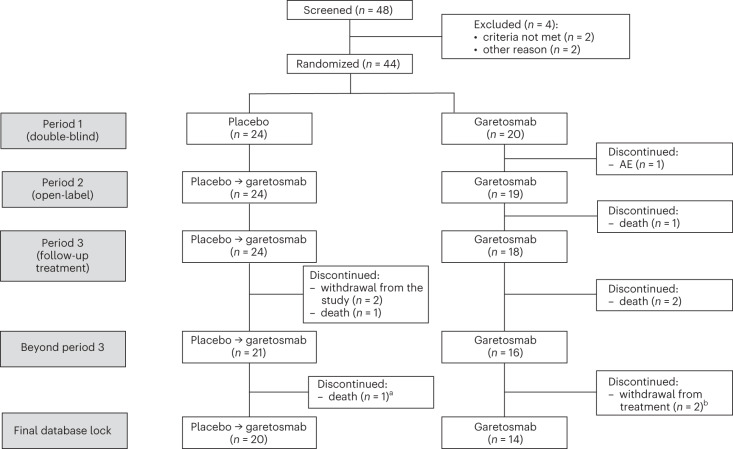
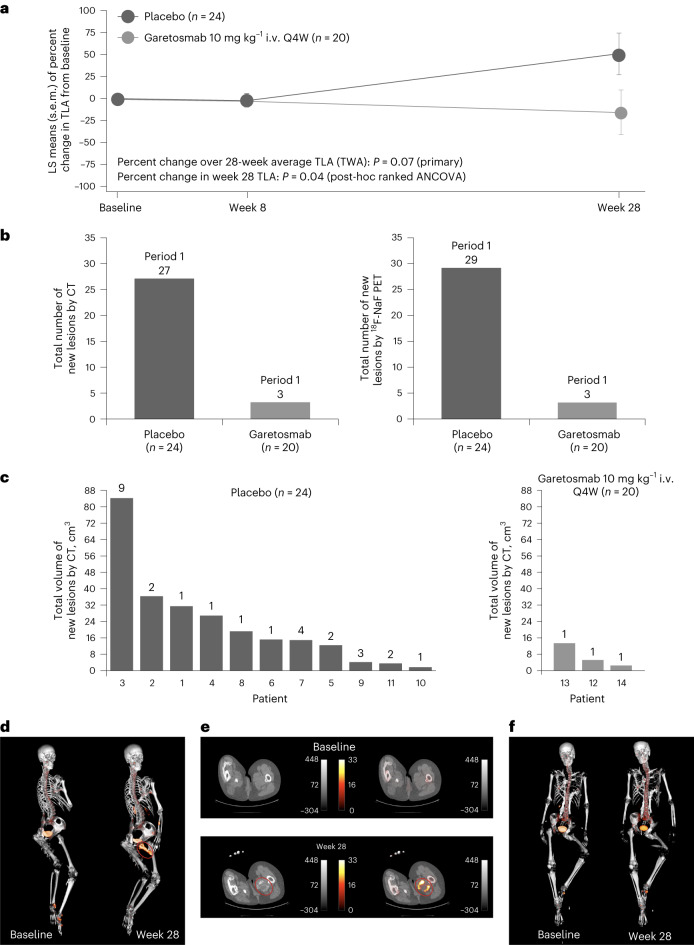
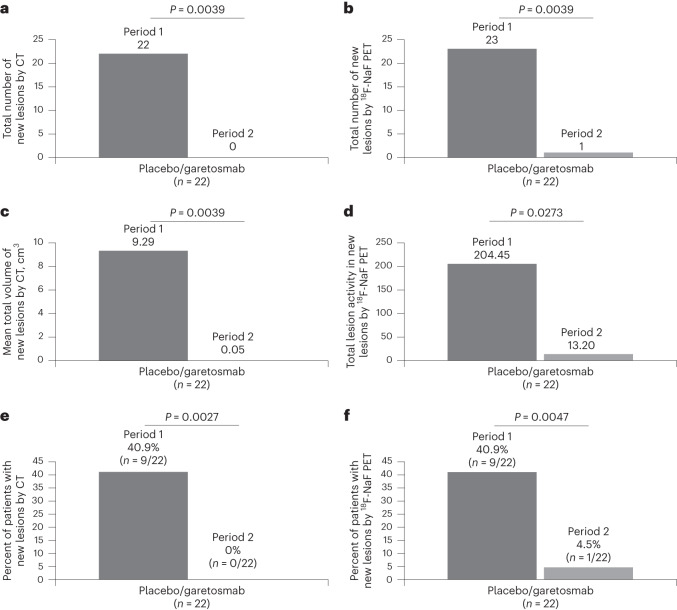
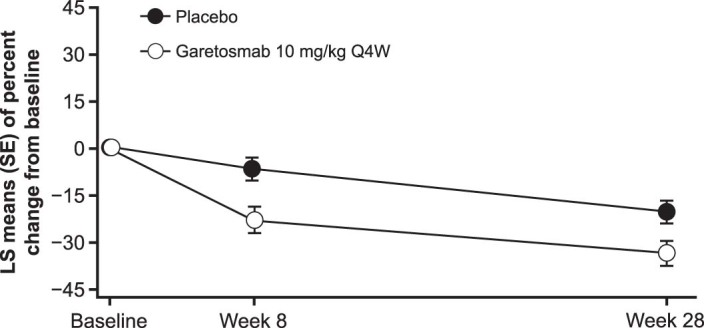
Fibrodysplasia ossificans progressiva (FOP) is a rare disease characterized by heterotopic ossification (HO) in connective tissues and painful flare-ups. In the phase 2 LUMINA-1 trial, adult patients with FOP were randomized to garetosmab, an activin A-blocking antibody (n = 20) or placebo (n = 24) in period 1 (28 weeks), followed by an open-label period 2 (28 weeks; n = 43). The primary end points were safety and for period 1, the activity and size of HO lesions. All patients experienced at least one treatment-emergent adverse event during period 1, notably epistaxis, madarosis and skin abscesses. Five deaths (5 of 44; 11.4%) occurred in the open-label period and, while considered unlikely to be related, causality cannot be ruled out. The primary efficacy end point in period 1 (total lesion activity by PET-CT) was not met (P = 0.0741). As the development of new HO lesions was suppressed in period 1, the primary efficacy end point in period 2 was prospectively changed to the number of new HO lesions versus period 1. No placebo patients crossing over to garetosmab developed new HO lesions (0% in period 2 versus 40.9% in period 1; P = 0.0027). Further investigation of garetosmab in FOP is ongoing. ClinicalTrials.gov identifier NCT03188666 .
© 2023. The Author(s).
Conflict of interest statement
M.D.R. is a principal investigator (PI) of Regeneron Pharmaceuticals and Ipsen trials. E.F.-N., C.P.-C., N.S., P.H., B.J.M., A.B., K.M., S.J.M., A.J.R., A.N.E., D.G.T., G.A.H., S.J.O., R.D., D.M.W. and G.D.Y. are employees of and hold stocks and shares in Regeneron Pharmaceuticals. R.J.P. is a PI of the Regeneron Pharmaceuticals LUMINA-1 and Clementia/Ipsen MOVE trials; a founding member and immediate past president of the International Clinical Council on FOP; and chair of the International Clinical Council Publications Committee. R.K. is a PI of clinical trials sponsored by Clementia/Ipsen and Regeneron Pharmaceuticals and is a non-paid member of the International Clinical Council on FOP and IFOPA registry advisory board. P.O. is a PI of clinical trials sponsored by Regeneron Pharmaceuticals. T.F.-B. is a sub-investigator of the Regeneron Pharmaceuticals LUMINA-1 trial and PI of IPSEN FALKON trial. C.R. has received research grants to their institution from Regeneron Pharmaceuticals. S.K. is a sub-investigator of the Regeneron Pharmaceuticals LUMINA-1 trial. A.M. is a sub-investigator in clinical trials sponsored by Regeneron Pharmaceuticals and Clementia-Ipsen. J.S.B. is a sub-investigator of the Regeneron Pharmaceuticals LUMINA-1 and Clementia/Ipsen MOVE trials. J.T. received grants to their institution (University Rzeszów) as a speaker for Merck and Novartis, and is a hired scientific expert for SoftSystem. M.S. is a speaker for Roche. J.B.-C. is an investigator of a clinical trial sponsored by Regeneron Pharmaceuticals. A.M.C. received a grant to their institution (University Health Network) for a clinical trial. K.M.D. is a PI on the Regeneron Pharmaceuticals LUMINA-1 trial. This project was supported by CTSA award no. UL1 TR002243 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors/sponsor and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health. E.B. is a sub-investigator of the Regeneron Pharmaceuticals LUMINA-1 trial at Amsterdam UMC, The Netherlands. P.G.R. is a sub-investigator of the Regeneron Pharmaceuticals LUMINA-1 trial at Amsterdam UMC, The Netherlands. M.A.M. is a PI of clinical trials sponsored by Clementia/Ipsen, Regeneron Pharmaceuticals and Incyte; and is a non-paid member of the International Clinical Council on FOP and IFOPA registry advisory board. L.T. received a grant to their institution (University Health Network) for a clinical trial (as a sub-investigator). E.M.W.E. receives subsidies/financing FOP research from the Dutch FOP Patient Foundation, IFOPA, Regeneron Pharmaceuticals, EU-IMI (AZ) and Clementia/Ipsen; holds non-paid board memberships for the International Clinical Council on FOP, IFOPA registry advisory board, Dutch Society for Endocrinology (NVE) BoNe; is a representative for Amsterdam Bone Center and Rare Bone Expert Center, European FOP consortium investigators; is a member of the ERN BOND and ASBMR committee; and is lead clinical PI on the Regeneron Pharmaceuticals LUMINA-1 trial. F.S.K. is a founding member and past president of the International Clinical Council on FOP; a member of the Medical Advisory Board of the IFOPA Global Registry; and a global PI on the Regeneron Pharmaceuticals LUMINA-1 and the Clementia/Ipsen MOVE trials.
Figures







References
-
- Liljesthrom M, Pignolo RJ, Kaplan FS. Epidemiology of the global fibrodysplasia ossificans progressiva (FOP) community. J. Rare Dis. Res Treat. 2020;5:31–36. doi: 10.29245/2572-9411/2020/2.1196. - DOI
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
