

Factors affecting the benefit of glasses alone in treating childhood amblyopia: an analysis of PEDIG data
- PMID: 37770832
- PMCID: PMC10540398
- DOI: 10.1186/s12886-023-03116-8
Factors affecting the benefit of glasses alone in treating childhood amblyopia: an analysis of PEDIG data
Erratum in
-
Correction: Factors affecting the benefit of glasses alone in treating childhood amblyopia: an analysis of PEDIG data.BMC Ophthalmol. 2023 Oct 24;23(1):432. doi: 10.1186/s12886-023-03170-2. BMC Ophthalmol. 2023. PMID: 37875877 Free PMC article. No abstract available.
Abstract
Background: To evaluate factors associated with better outcomes from optical treatment alone in amblyopic children from 3 up to 7 years.
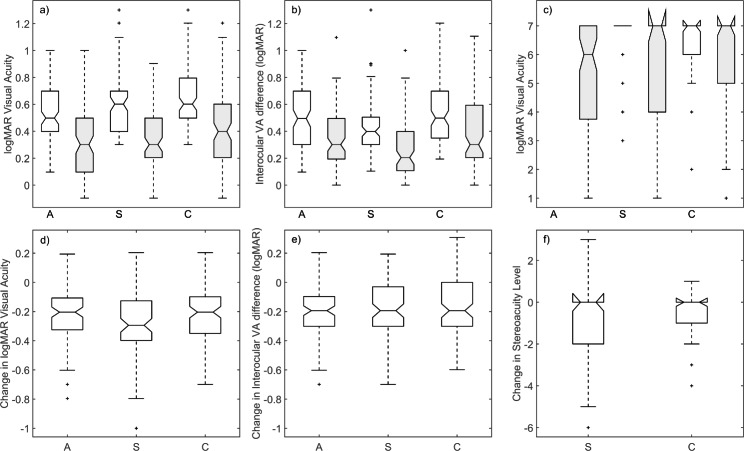
Methods: Data extracted from two studies with similar protocols, Amblyopic Treatment Studies 5 (n = 152) and 13 (n = 128) from the Pediatric Eye Disease Investigator Group database, were used to determine by regression analysis the factors associated with improvements in visual acuity in the amblyopic eye, inter-ocular visual acuity difference and stereoacuity. Input variables were aetiology of amblyopia (anisometropic, strabismic and combined-mechanism amblyopia), treatment compliance, visual acuity, interocular visual acuity difference, stereoacuity, tropia size at distance and near, age and refractive error at baseline.
Results: Despite the range of clinical factors considered, our models explain only a modest proportion of the variance in optical treatment outcomes. The better predictors of the degree of optical treatment success in amblyopic children are visual acuity of the amblyopic eye, interocular visual acuity difference, stereoacuity, treatment compliance and the amblyopic eye spherical-equivalent refractive error. While the aetiology of the amblyopia does not exert a major influence upon treatment outcome, combined-mechanism amblyopes experience the smallest improvement in visual acuity, tropia and stereoacuity and may need longer optical treatment periods.
Conclusions: While results identify the factors influencing optical treatment outcome in amblyopic children, clinicians will be unable to predict accurately the benefits of optical treatment in individual patients. Whether this is because relevant clinical or non-clinical factors (e.g. nature and volume of daily activities undertaken) influences the outcomes from optical treatment has not yet been identified and remains to be discovered.
The specific benefit of optical correction is already established and this has led to a change in amblyopia management whereby treatment starts with the provision of optical correction alone.
The best predictors of the degree of optical treatment success in amblyopic children are visual acuity of the amblyopic eye, interocular visual acuity difference, stereoacuity, treatment compliance and the amblyopic eye spherical-equivalent refractive error.
Overall, optical treatment alone resolved amblyopia in a low percentage of the amblyopic children. Furthermore, based on statistical modelling, clinicians will not be able to predict accurately the benefits of optical treatment for each individual patient.
Keywords: Amblyopia; Interocular difference; Optical treatment; Stereoacuity; Visual acuity.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declares that they have no competing interest. The authors declare that they have no conflict of interest. The authors declare that this work has not received any financial support.
Figures



References
-
- Ciuffreda KJ, Levi DM, Selenow A. Amblyopia: basic and clinical aspects. United States: Butterworth-Heinemann; 1991.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
