

A comparative study on the clinical efficacy of microplate trans-carpometacarpal joint fixation and non-trans-carpometacarpal joint fixation in treating fractures with dislocation or subluxation of the base of the fourth and fifth metacarpal bones
- PMID: 37770964
- PMCID: PMC10540348
- DOI: 10.1186/s13018-023-04225-2
A comparative study on the clinical efficacy of microplate trans-carpometacarpal joint fixation and non-trans-carpometacarpal joint fixation in treating fractures with dislocation or subluxation of the base of the fourth and fifth metacarpal bones
Abstract
Background: This study aimed to compare the clinical efficacy of microplate trans-carpometacarpal joint fixation and non-trans-carpometacarpal joint fixation in treating fractures and dislocation or subluxation of the base of the fourth and fifth metacarpal bones.
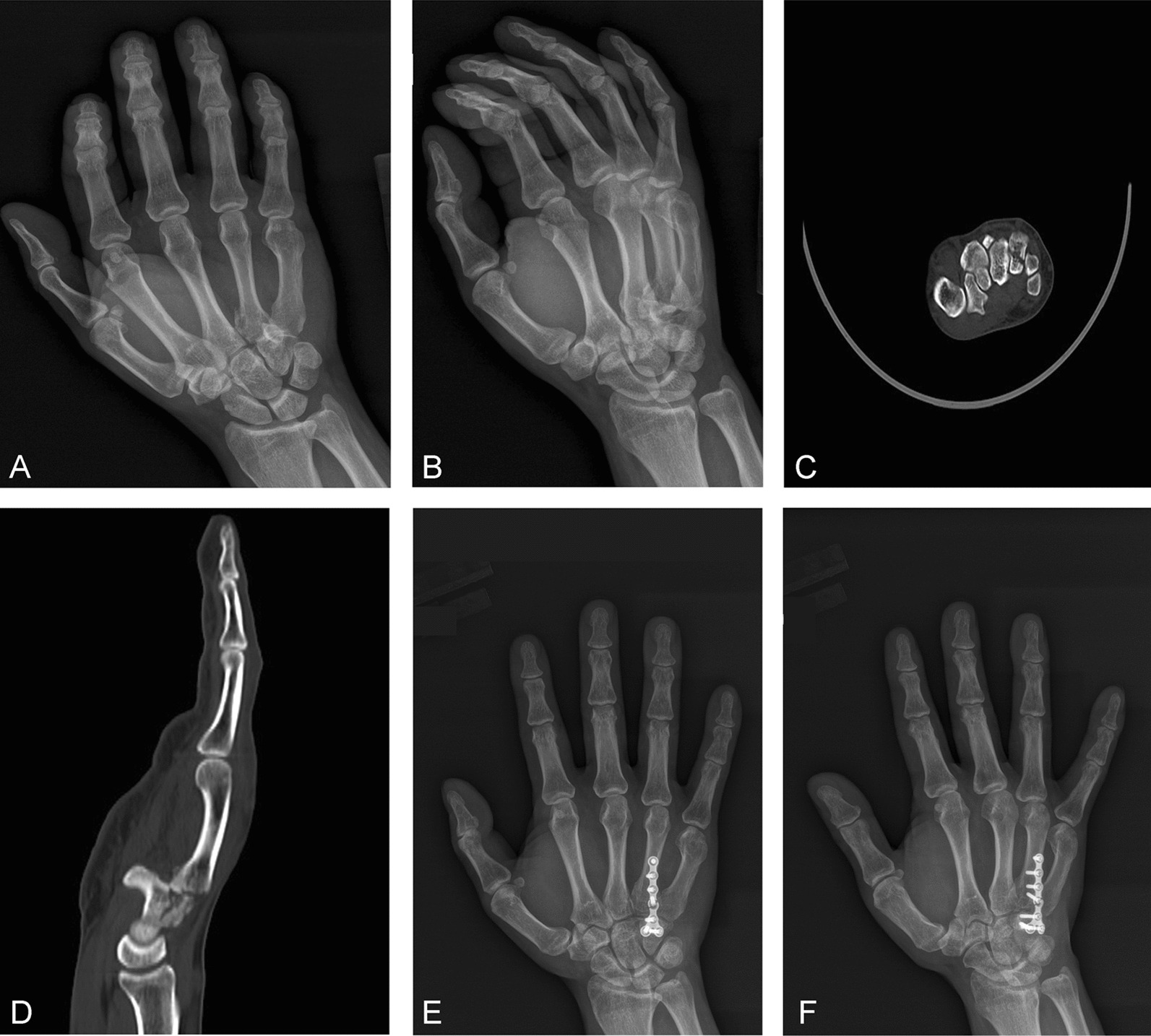
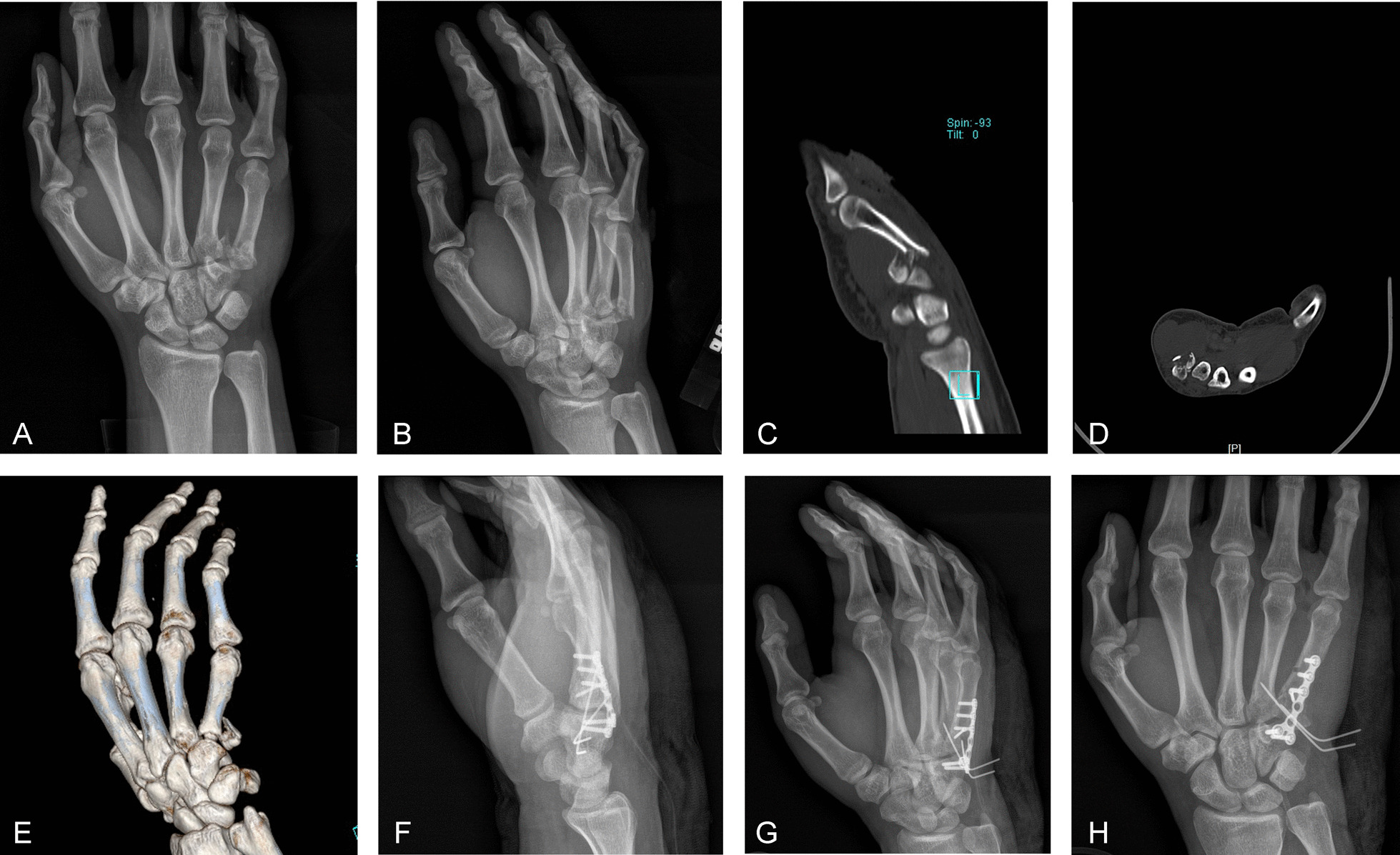
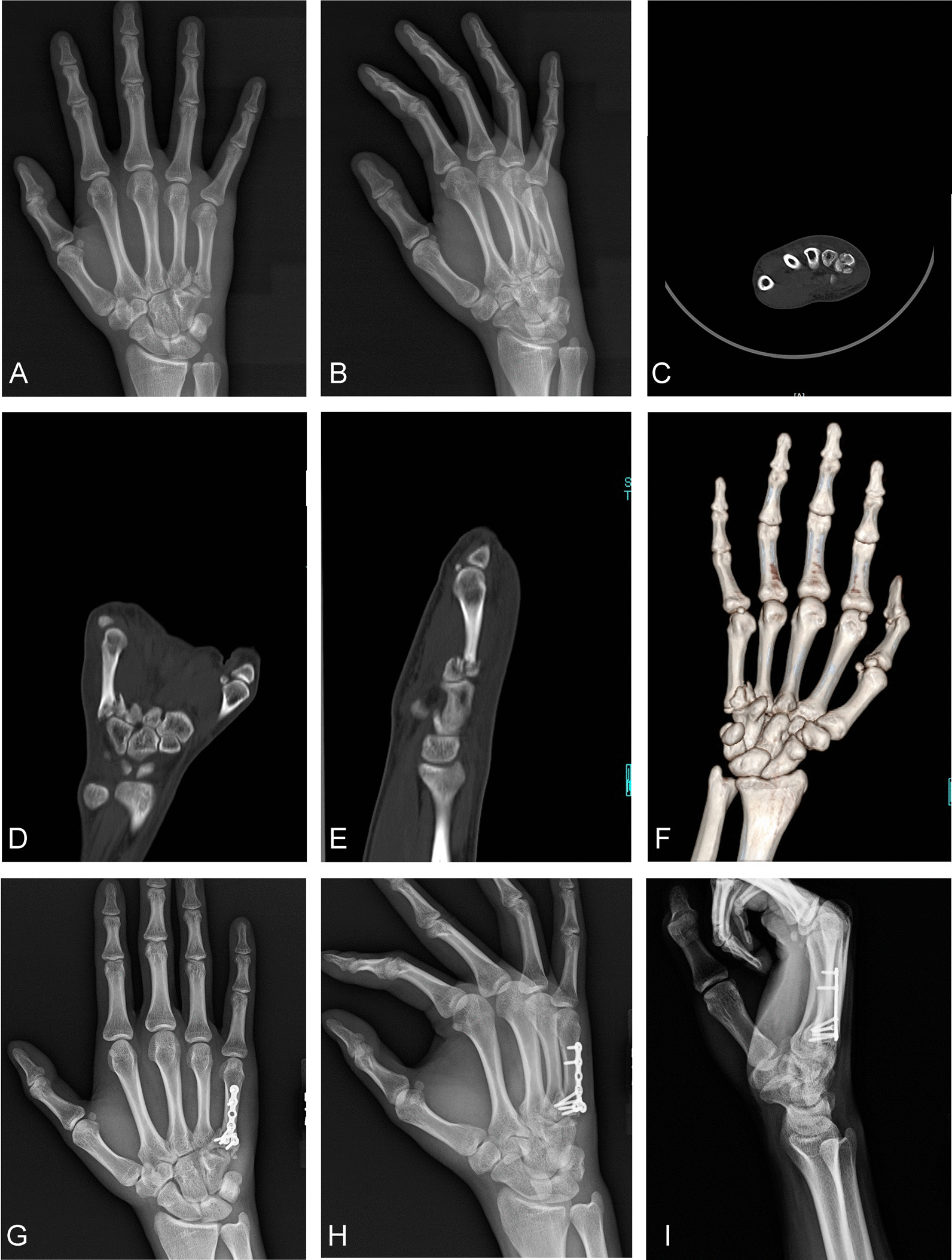
Method: From 2015 to 2021, 100 cases of metacarpal basal fractures with dislocation or subluxation were randomly divided into the trans-carpometacarpal joint fixation group (group A) and non-trans-carpometacarpal joint fixation group (group B). Group A (n = 50) comprised 44 males and 6 females, with an average age of 28.8 ± 6.1 y and an Orthopedic Trauma Association (OTA) fracture classification of type B1 (n = 29) or C1 (n = 21). Group B (n = 50) comprised 45 males and 5 females, with an average age of 28.9 ± 5.7 y and an OTA fracture classification of type B1 (n = 28) or C1 (n = 22). All patients were complicated with dislocation or subluxation. The surgery time, fracture healing time, postoperative handgrip strength, and total active motion (TAM) scores of the ring and little fingers were recorded and compared between the two groups. The clinical efficacy of patients was evaluated using scoring methods such as DASH (disabilities of the arm, shoulder and hand), visual analogue scale (VAS), and Mayo at 3, 6, and 12 months after surgery.
Results: There was no significant difference in the general indexes, surgery time, or fracture healing time between the two groups (P > 0.05). There were no significant differences in handgrip strength and TAM scores of the ring and little fingers between the two groups at 3 and 12 months postoperatively (P > 0.05), but there were significant differences in these indexes 6 months postoperatively (P < 0.05). There were no significant differences in the DASH, VAS, and Mayo scores at 3 and 12 months postoperatively (P > 0.05), but there were significant differences between the two groups in the DASH and Mayo scores (P < 0.05) but not the VAS score (P > 0.05) 6 months postoperatively.
Conclusion: In the treatment of fourth and fifth metacarpal basal fractures with dislocation or subluxation, both microplate transarticular fixation and non-transarticular fixation could achieve fracture fixation and healing, and each method had advantages and disadvantages. The clinically appropriate fixation method should be selected according to the experience of the surgeon and the degree and type of fracture and dislocation.
Keywords: Carpometacarpal joint; Fracture and dislocation; Fracture fixation; Hand; Metacarpal base.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
[Mini locked-plate trans-carpometacarpal joint internal fixation for treating comminuted fracture of base of the fifth metacarpal].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 Nov 15;32(11):1382-1385. doi: 10.7507/1002-1892.201805077. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 30417611 Free PMC article. Chinese.
-
Comparison of plaster cast and open reduction internal fixation in delayed fourth and fifth carpometacarpal fracture-dislocations.Jt Dis Relat Surg. 2023 Apr 26;34(2):315-324. doi: 10.52312/jdrs.2023.851. Jt Dis Relat Surg. 2023. PMID: 37462634 Free PMC article.
-
Hamate metacarpal injury: a case series and suggested algorithm for treatment.Eur J Orthop Surg Traumatol. 2025 Apr 9;35(1):151. doi: 10.1007/s00590-025-04275-8. Eur J Orthop Surg Traumatol. 2025. PMID: 40202612
-
Coronal Hamate Fracture Associated With Carpometacarpal Dislocations of All of the Fingers: Review of the Literature and Case Report.Hand (N Y). 2017 Sep;12(5):NP51-NP54. doi: 10.1177/1558944716668860. Epub 2016 Sep 22. Hand (N Y). 2017. PMID: 28832201 Free PMC article. Review.
-
"Stabilized arthroplasty" for old fracture dislocations of the fifth carpometacarpal joint.Tech Hand Up Extrem Surg. 2009 Sep;13(3):134-6. doi: 10.1097/BTH.0b013e3181aa25c4. Tech Hand Up Extrem Surg. 2009. PMID: 19730041 Review.
Cited by
-
Changes in serum NO, ET-1, and VEGF after cannulated screw fixation in patients with femoral neck fractures and their relationship with femoral head necrosis.Front Physiol. 2025 Jul 23;16:1603323. doi: 10.3389/fphys.2025.1603323. eCollection 2025. Front Physiol. 2025. PMID: 40771454 Free PMC article.
References
-
- Valent L, Sousa A, Goncalves AM, et al. Facture of the hamate with carpometacarpal dislocation. Acta Med Port. 2007;20(2):179–184. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
