

Systems immunology-based drug repurposing framework to target inflammation in atherosclerosis
- PMID: 37771373
- PMCID: PMC10538622
- DOI: 10.1038/s44161-023-00278-y
Systems immunology-based drug repurposing framework to target inflammation in atherosclerosis
Erratum in
-
Erratum: Publisher Correction: Systems immunology-based drug repurposing framework to target inflammation in atherosclerosis.Nat Cardiovasc Res. 2023;2(8):793. doi: 10.1038/s44161-023-00310-1. Epub 2023 Jul 4. Nat Cardiovasc Res. 2023. PMID: 38666036 Free PMC article.
Abstract
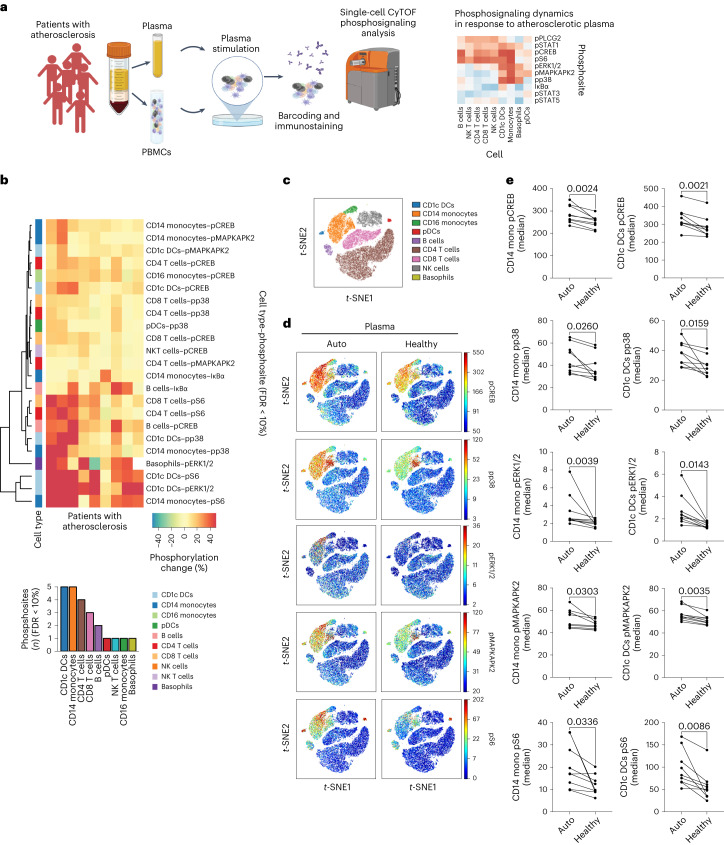
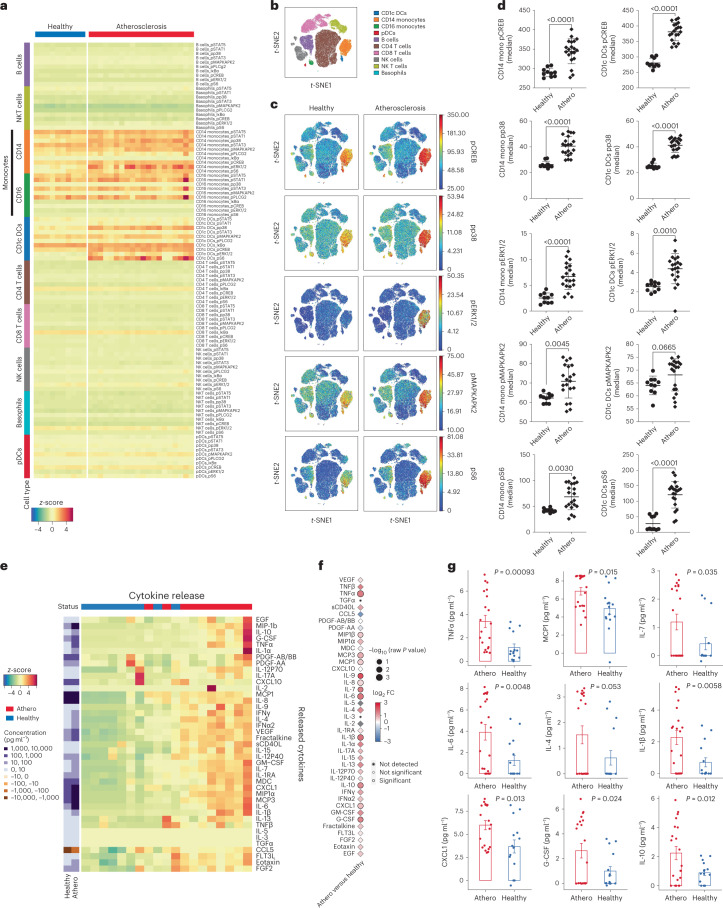
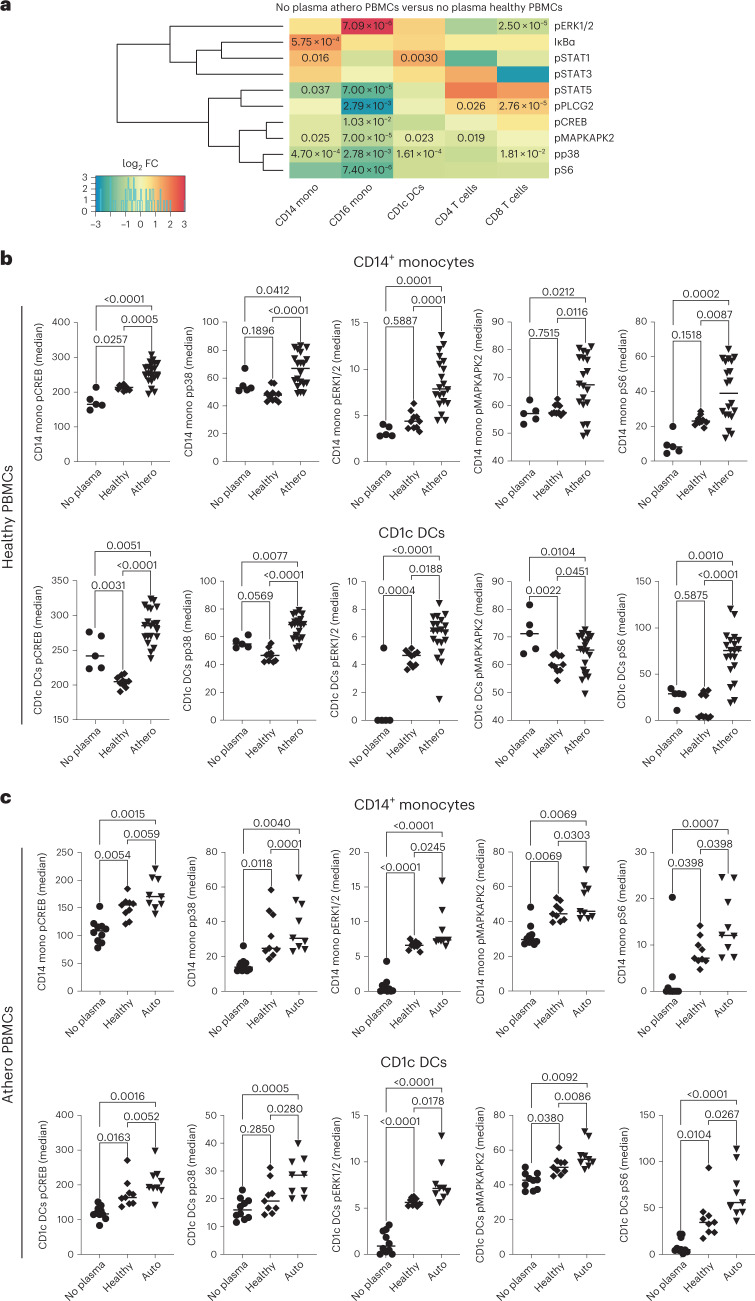
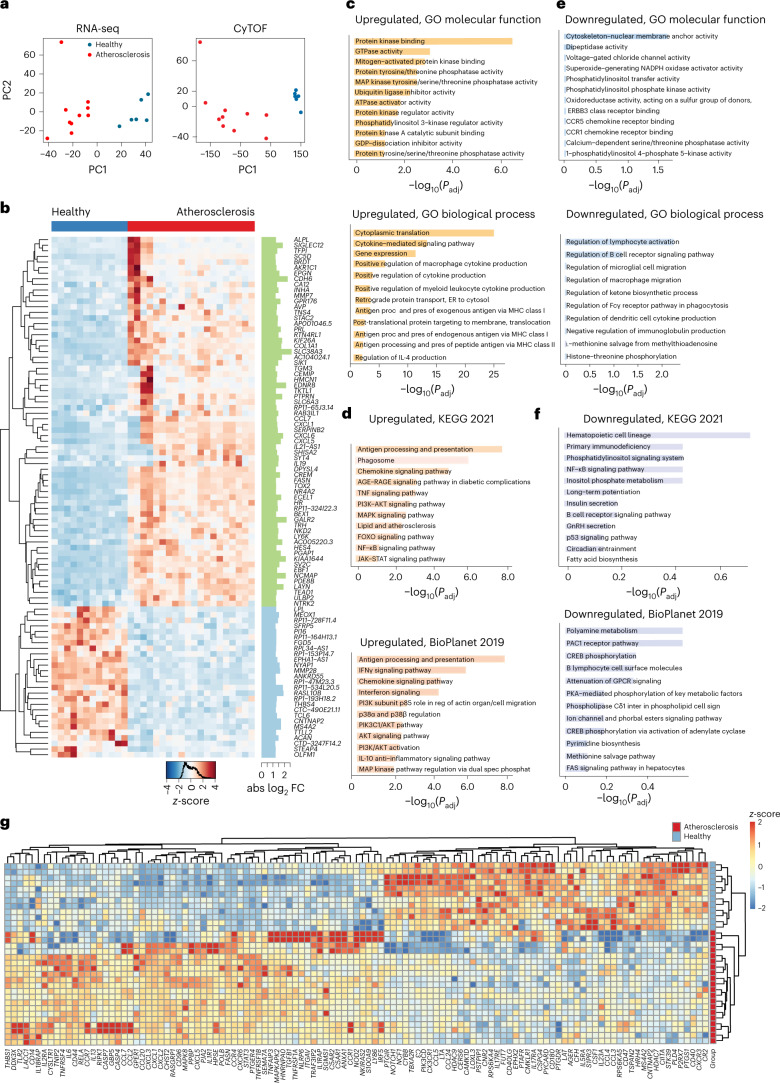
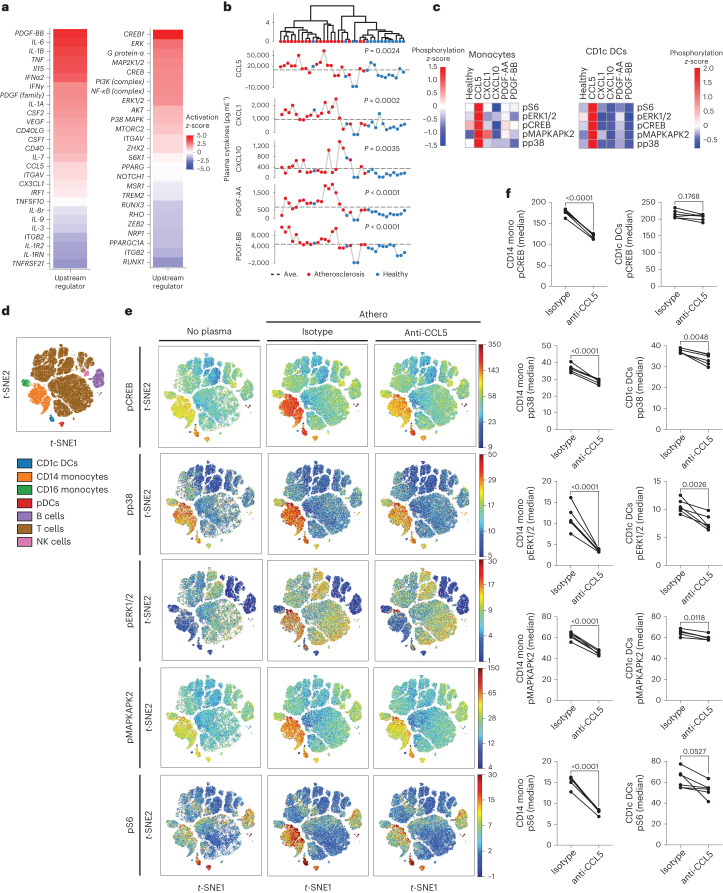
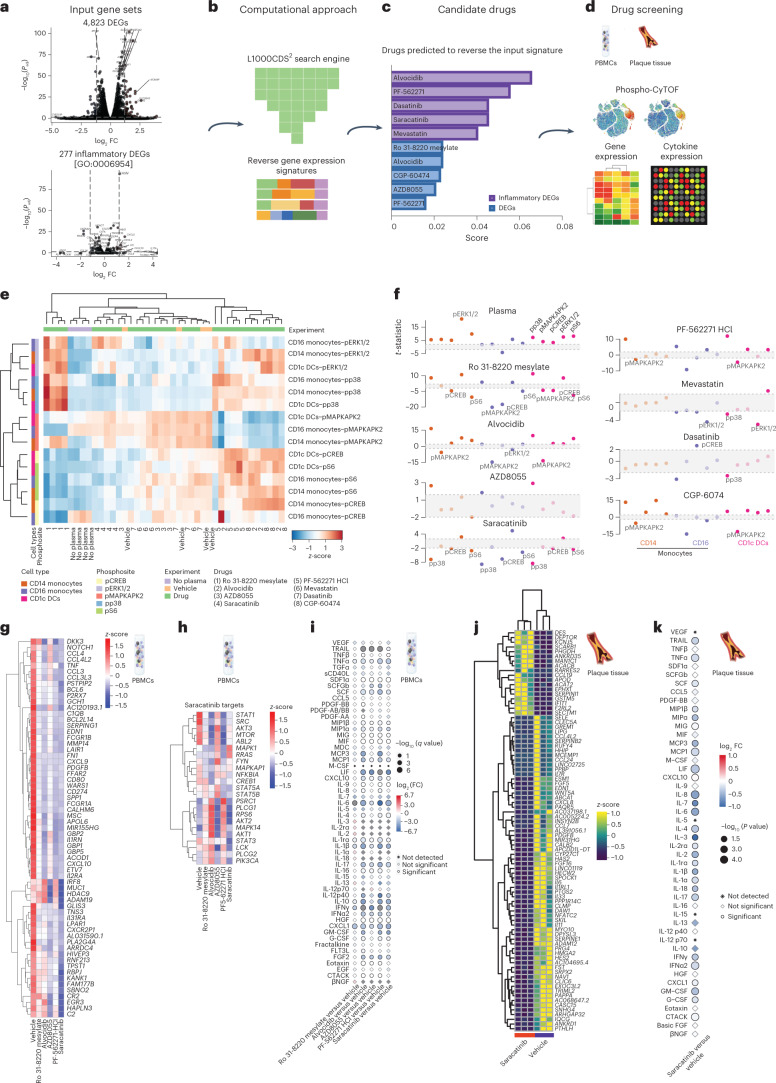
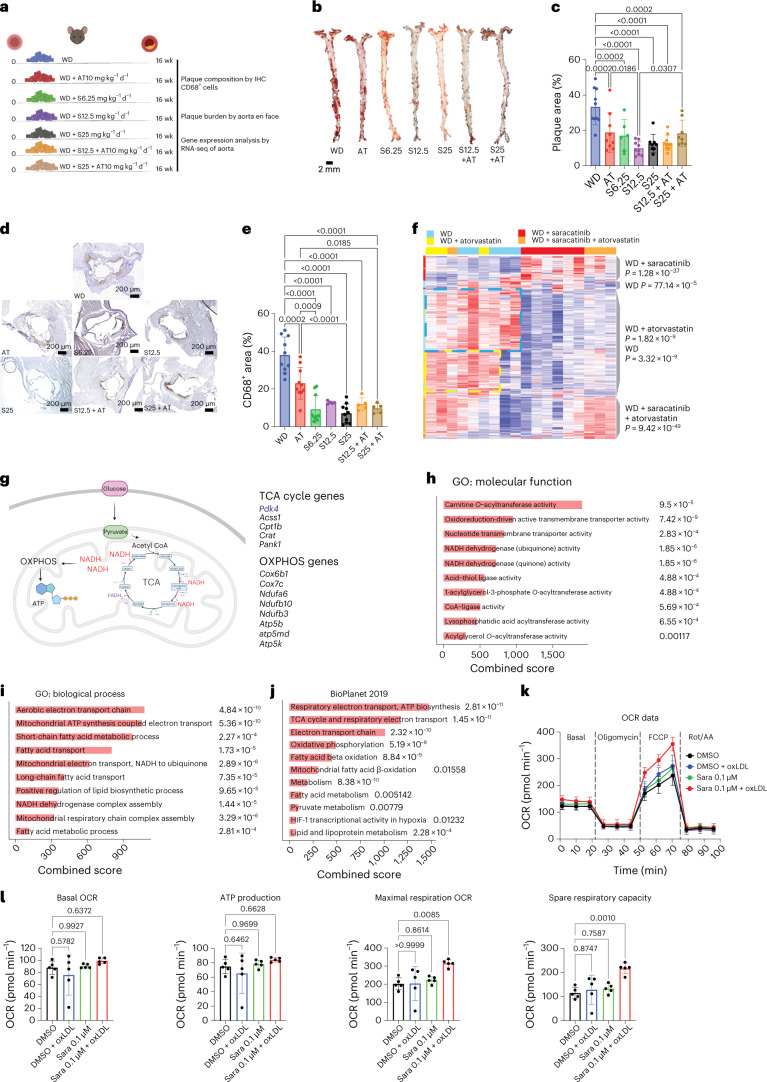
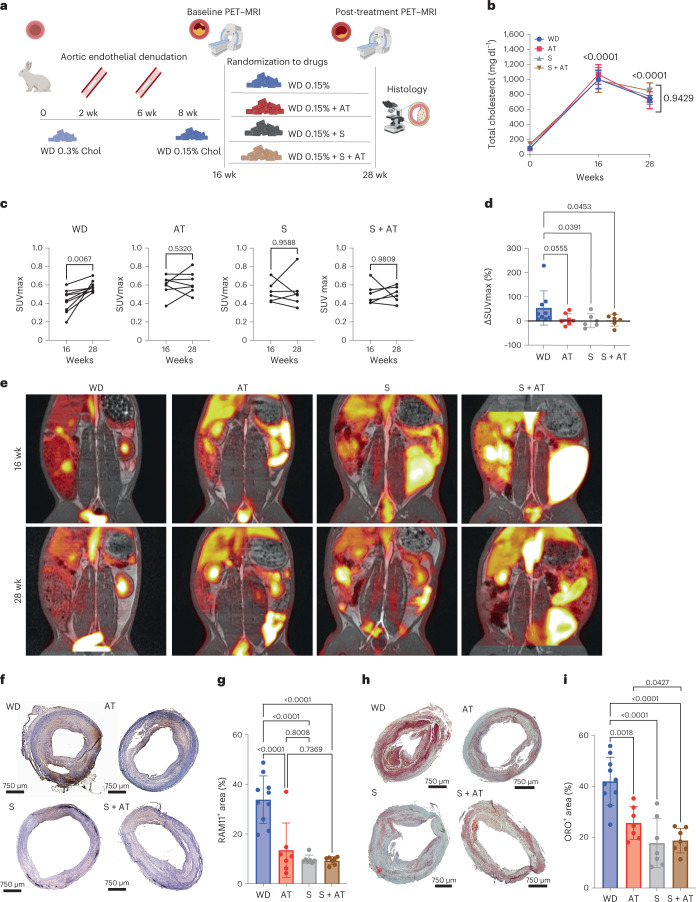
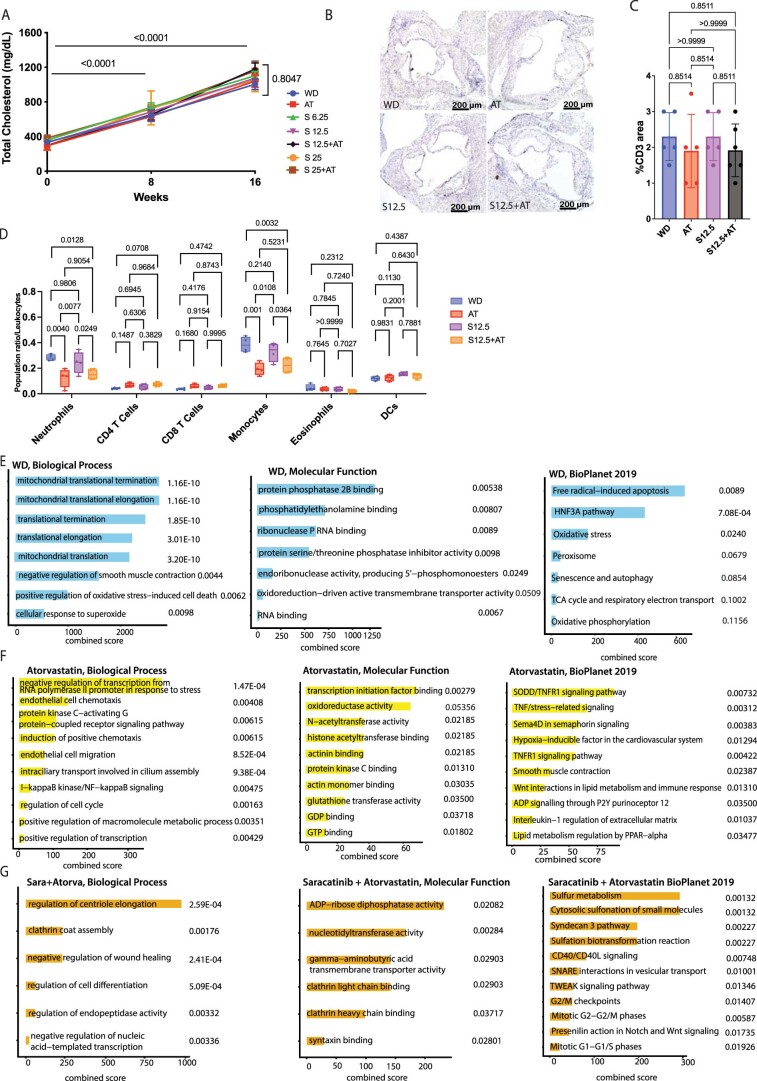
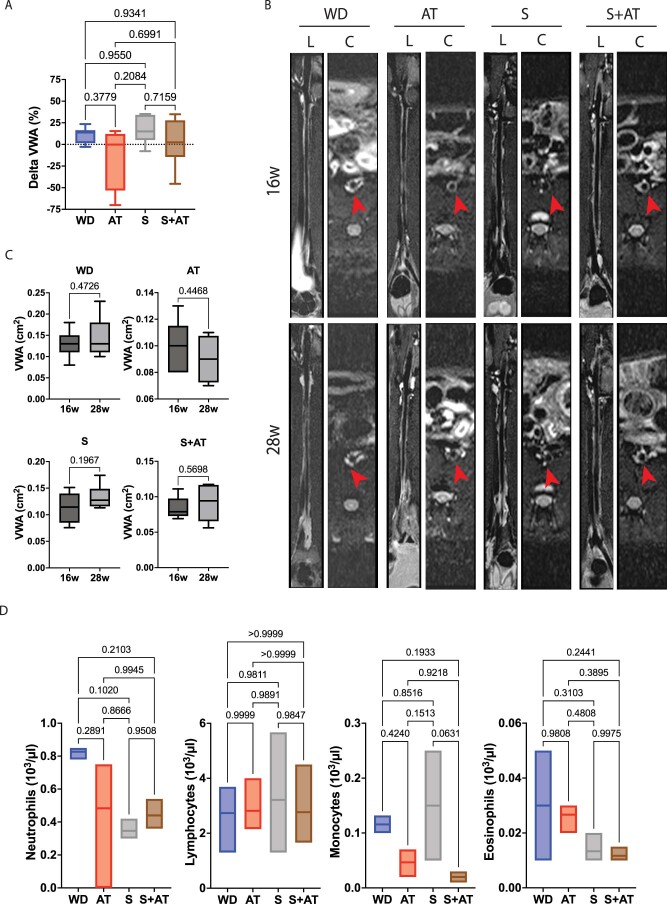
The development of new immunotherapies to treat the inflammatory mechanisms that sustain atherosclerotic cardiovascular disease (ASCVD) is urgently needed. Herein, we present a path to drug repurposing to identify immunotherapies for ASCVD. The integration of time-of-flight mass cytometry and RNA sequencing identified unique inflammatory signatures in peripheral blood mononuclear cells stimulated with ASCVD plasma. By comparing these inflammatory signatures to large-scale gene expression data from the LINCS L1000 dataset, we identified drugs that could reverse this inflammatory response. Ex vivo screens, using human samples, showed that saracatinib-a phase 2a-ready SRC and ABL inhibitor-reversed the inflammatory responses induced by ASCVD plasma. In Apoe-/- mice, saracatinib reduced atherosclerosis progression by reprogramming reparative macrophages. In a rabbit model of advanced atherosclerosis, saracatinib reduced plaque inflammation measured by [18F] fluorodeoxyglucose positron emission tomography-magnetic resonance imaging. Here we show a systems immunology-driven drug repurposing with a preclinical validation strategy to aid the development of cardiovascular immunotherapies.
Conflict of interest statement
Competing Interests statement C.G. is listed as an inventor on patent application Tech 160808G PCT/US2022/017777, filed by the Icahn School of Medicine at Mount Sinai (patent applicant), that is directly related to the method used in this manuscript to identify saracatinib as an antiatherosclerotic agent. The remaining authors declare no competing interests.
Figures
References
Grants and funding
- P01 HL131481/HL/NHLBI NIH HHS/United States
- UH2 TR002067/TR/NCATS NIH HHS/United States
- U54 HL127624/HL/NHLBI NIH HHS/United States
- UH3 TR002067/TR/NCATS NIH HHS/United States
- OT2 OD030160/OD/NIH HHS/United States
- R21 TR001739/TR/NCATS NIH HHS/United States
- T32 HL007824/HL/NHLBI NIH HHS/United States
- RC2 DK131995/DK/NIDDK NIH HHS/United States
- R01 HL143814/HL/NHLBI NIH HHS/United States
- R35 HL135799/HL/NHLBI NIH HHS/United States
- R01 DK131525/DK/NIDDK NIH HHS/United States
- R01 HL153712/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous