

Phase II trial of concurrent sunitinib, temozolomide, and radiotherapy with adjuvant temozolomide for newly diagnosed MGMT unmethylated glioblastoma
- PMID: 37771465
- PMCID: PMC10530294
- DOI: 10.1093/noajnl/vdad106
Phase II trial of concurrent sunitinib, temozolomide, and radiotherapy with adjuvant temozolomide for newly diagnosed MGMT unmethylated glioblastoma
Abstract
Background: The overall prognosis of glioblastoma (GBM) remains dismal, particularly for patients with unmethylated O6-methylguanine-DNA-methyltransferase (MGMT) promoter. In this phase II trial, we tested the combination of the antiangiogenic agent sunitinib with radiotherapy and temozolomide (TMZ) for newly diagnosed unmethylated MGMT GBM patients.
Methods: We enrolled 37 patients with unmethylated MGMT promoter GBM, age 18-70, and KPS ≥70. Patients received 12.5 mg of daily sunitinib for 7 days, followed by concurrent chemoradiation plus 12.5 mg sunitinib, then adjuvant TMZ. The primary endpoint was progression-free survival (PFS), and secondary endpoints were overall survival (OS), safety, and neutrophil-to-lymphocyte ratio (NLR) biomarker.
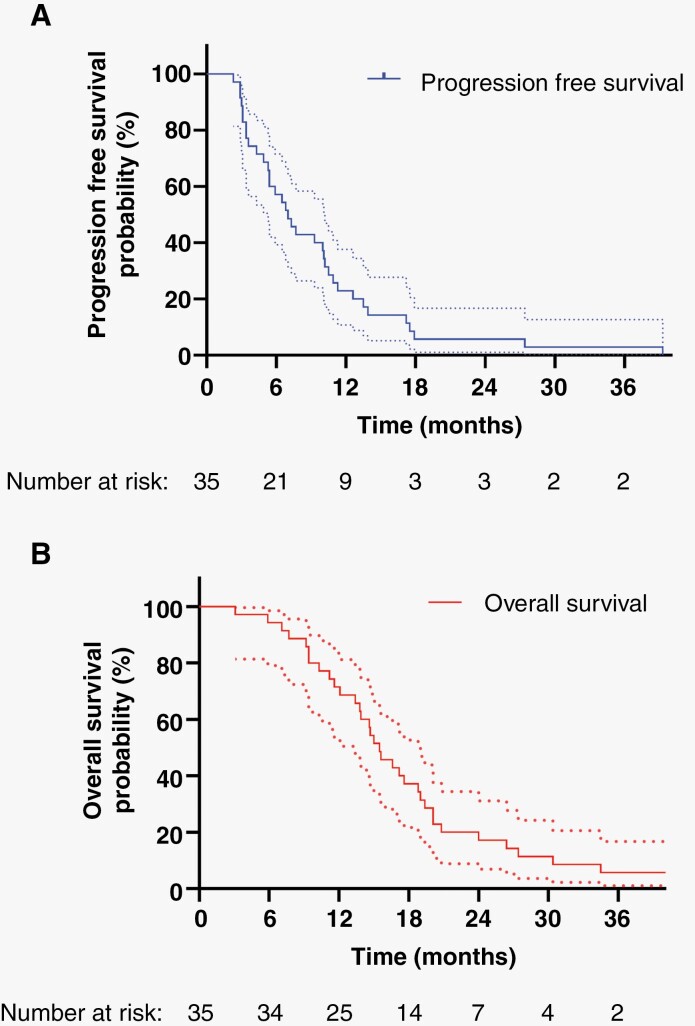
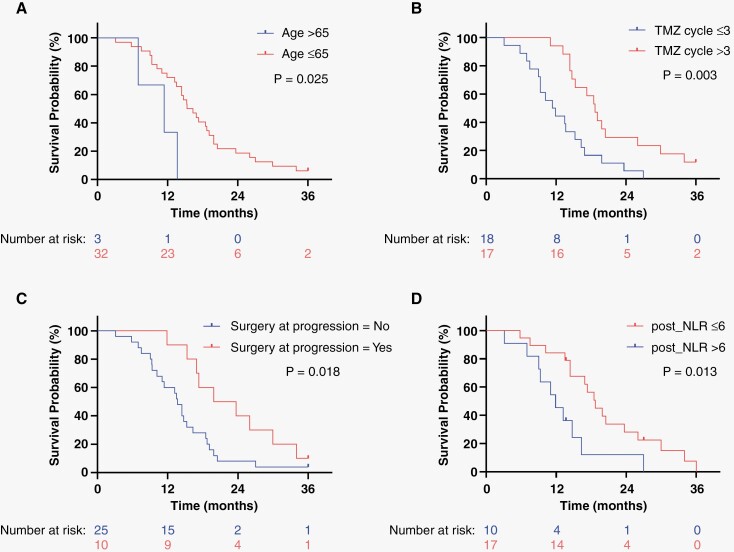
Results: At a median follow-up time of 15.3 months (range: 3.1-71.3 months), the median PFS was 7.15 months (95% CI: 5.4-10.5) and the 6-month PFS was 54.0%. Median OS was 15.0 months (95% CI: 13.8-19.4) and 2-year OS rate was 17.1%. Patients receiving >3 cycles of adjuvant TMZ, undergoing surgery at progression, and presenting a post-concurrent NLR ≤6 experienced a significant improved OS with hazard ratios of 0.197 (P = .001), 0.46 (P = .049), and 0.38 (P = .021), respectively, on multivariable analysis. Age >65 years predicted for worse OS with hazard ratio of 3.92 (P = .037). Grade ≥3 thrombocytopenia occurred in 22.9%, grade ≥3 neutropenia in 20%, and grade ≥3 thromboembolic events in 14.3% of patients. There were no grade 5 events.
Conclusion: Our findings suggest a potential benefit of combining sunitinib with chemoradiation in newly diagnosed GBM patients with unmethylated MGMT status and provide a strong rationale to test this combination in future studies.
Keywords: glioblastoma; radiation therapy; sunitinib; temozolomide; unmethylated MGMT.
© The Author(s) 2023. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
None declared. Pfizer provided funding but was not involved in the design, recruitment, and analysis of data in this clinical trial.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. - PubMed
-
- Laperriere N, Zuraw L, Cairncross G; Cancer Care Ontario Practice Guidelines Initiative Neuro-Oncology Disease Site G. Radiotherapy for newly diagnosed malignant glioma in adults: a systematic review. Radiother Oncol. 2002;64(3):259–273. - PubMed
-
- Paszat L, Laperriere N, Groome P, et al. . A population-based study of glioblastoma multiforme. Int J Radiat Oncol Biol Phys. 2001;51(1):100–107. - PubMed
-
- Hegi ME, Diserens AC, Gorlia T, et al. . MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352(10):997–1003. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials