

Adding Family Digital Supports to Classroom-Based Physical Activity Interventions to Target In- and Out-of-School Activity: An Evaluation of the Stay Active Intervention during the COVID-19 Pandemic
- PMID: 37771566
- PMCID: PMC10522008
Adding Family Digital Supports to Classroom-Based Physical Activity Interventions to Target In- and Out-of-School Activity: An Evaluation of the Stay Active Intervention during the COVID-19 Pandemic
Abstract
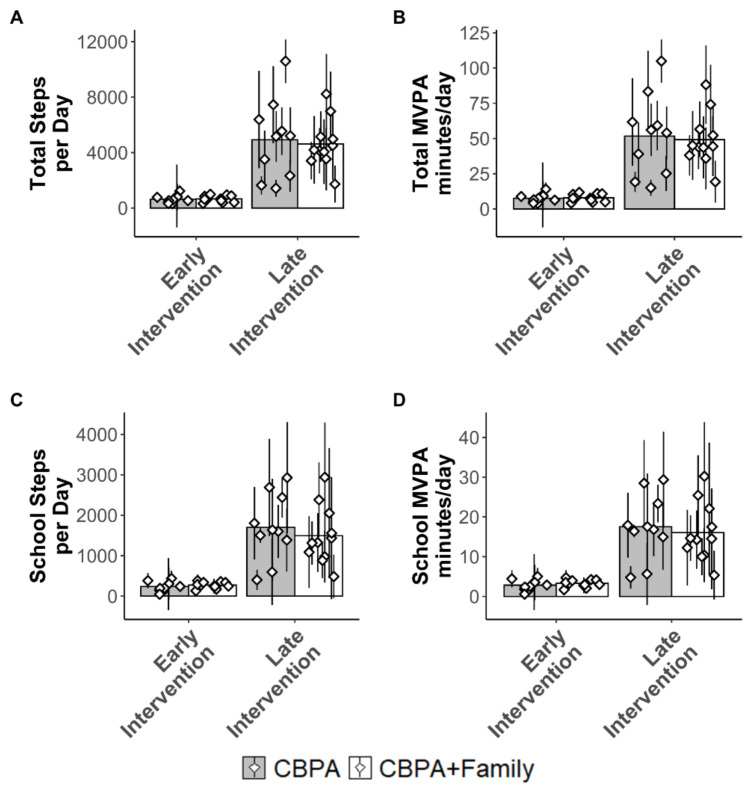
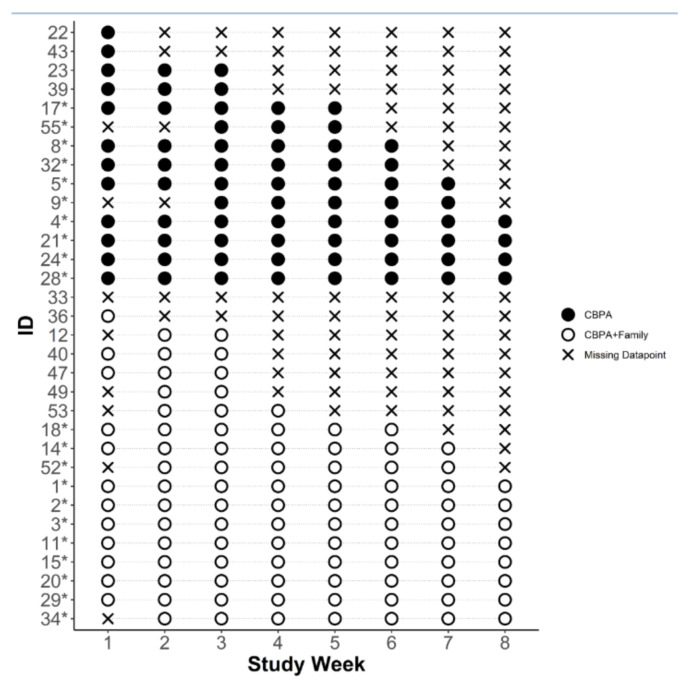
Remotely delivered interventions are promising for reaching large numbers of people, though few have targeted multiple levels of influence such as schools and families. This study evaluated two versions (arms) of a remotely delivered classroom-based physical activity (CBPA) intervention. One arm solely included remote CBPA; the other included remote CBPA and mobile health (mHealth) family supports. Six schools were randomized to CBPA or CBPA+Family. Both arms were remotely delivered for seven weeks. CBPA+Family added behavior change tools delivered via text messages and newsletters to caregiver/child dyads. Garmin devices measured moderate-to-vigorous activity (MVPA) in both arms and were used for goal setting/ monitoring in the CBPA+Family arm (integrated with the text messages). Caregivers completed surveys evaluating intervention acceptability. 53 participants (CBPA n=35; CBPA+Family n=18; 9.7±0.7 years) were included. Increases in MVPA were similar between arms, showing a pre-post effect of the CBPA but no additional effect of family supports. MVPA was low at baseline and during the first 3 weeks (CBPA 7.5±3.1 minutes/day; CBPA+Family 7.9±2.7 minutes/day) and increased by Weeks 6-8 (CBPA 56.8±34.2 minutes/day; CBPA+Family 49.2±18.7 minutes/day). Approximately 90% of caregivers reported high satisfaction with the added family support content. CBPA+Family participants wore the Garmin later into the study period. Remote delivery of CBPA appears feasible and effective for supporting increases in children's MVPA. Adding family supports to school-based interventions appears acceptable and may support engagement, demonstrating promise for more multilevel/multi-setting interventions, though the multilevel intervention was not more effective than the single-level intervention in increasing children's MVPA.
Keywords: mHealth; mobile health; pediatric; school; short messaging system (SMS); wearables.
© JHEAL, 2021.
Conflict of interest statement
Conflicts of interest: All authors report no conflicts of interest.
Figures

Similar articles
-
Interventions in outside-school hours childcare settings for promoting physical activity amongst schoolchildren aged 4 to 12 years.Cochrane Database Syst Rev. 2021 Sep 27;9(9):CD013380. doi: 10.1002/14651858.CD013380.pub2. Cochrane Database Syst Rev. 2021. PMID: 34694005 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
The Impact of an Adaptive mHealth Intervention on Improving Patient-Provider Health Care Communication: Secondary Analysis of the DIAMANTE Trial.JMIR Mhealth Uhealth. 2025 Jul 17;13:e64296. doi: 10.2196/64296. JMIR Mhealth Uhealth. 2025. PMID: 40674692 Free PMC article. Clinical Trial.
-
Effectiveness and Implementation of a Text Messaging mHealth Intervention to Prevent Childhood Obesity in Mexico in the COVID-19 Context: Mixed Methods Study.JMIR Mhealth Uhealth. 2024 Apr 9;12:e55509. doi: 10.2196/55509. JMIR Mhealth Uhealth. 2024. PMID: 38592753 Free PMC article. Clinical Trial.
-
Interventions to prevent obesity in children aged 5 to 11 years old.Cochrane Database Syst Rev. 2024 May 20;5(5):CD015328. doi: 10.1002/14651858.CD015328.pub2. Cochrane Database Syst Rev. 2024. PMID: 38763517 Free PMC article.
Cited by
-
Moderate-to-vigorous intensity physical activity among U.S. adolescents before and during the COVID-19 pandemic: Findings from the Adolescent Brain Cognitive Development Study.Prev Med Rep. 2023 Jul 23;35:102344. doi: 10.1016/j.pmedr.2023.102344. eCollection 2023 Oct. Prev Med Rep. 2023. PMID: 37564120 Free PMC article.
References
-
- Brazendale K, Beets MW, Weaver RG, Pate RR, Turner-McGrievy GM, Kaczynski AT... & von Hippel PT. Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis. International Journal of Behavioral Nutrition and Physical Activity. 2017;14(1):1–14. - PMC - PubMed
-
- Carlson JA, Engelberg JK, Cain KL, Conway TL, Mignano AM, Bonilla EA, Sallis JF. Implementing classroom physical activity breaks: Associations with student physical activity and classroom behavior. Preventive medicine. 2015;81:67–72. - PubMed
LinkOut - more resources
Full Text Sources