

Automated advanced imaging in acute ischemic stroke. Certainties and uncertainties
- PMID: 37771657
- PMCID: PMC10523426
- DOI: 10.1016/j.ejro.2023.100524
Automated advanced imaging in acute ischemic stroke. Certainties and uncertainties
Abstract
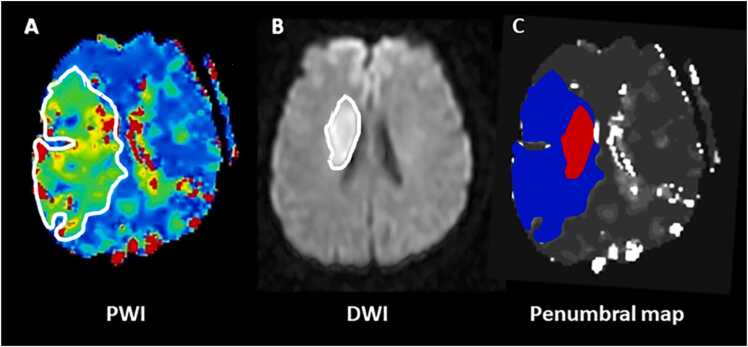
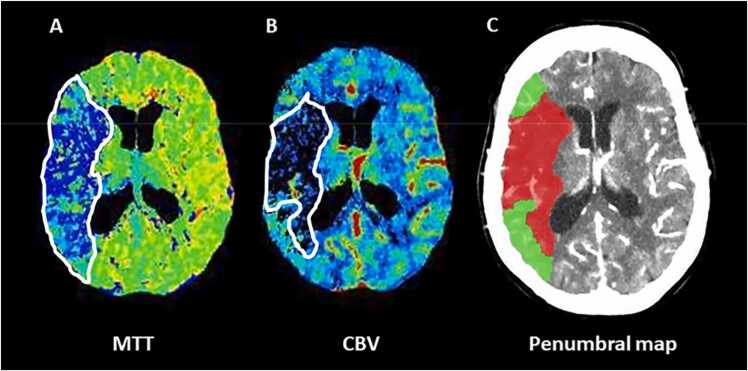
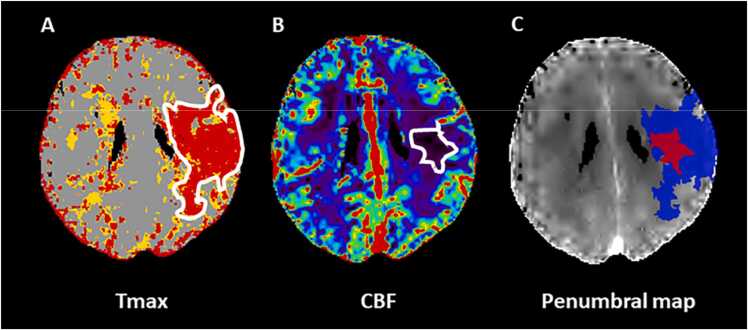
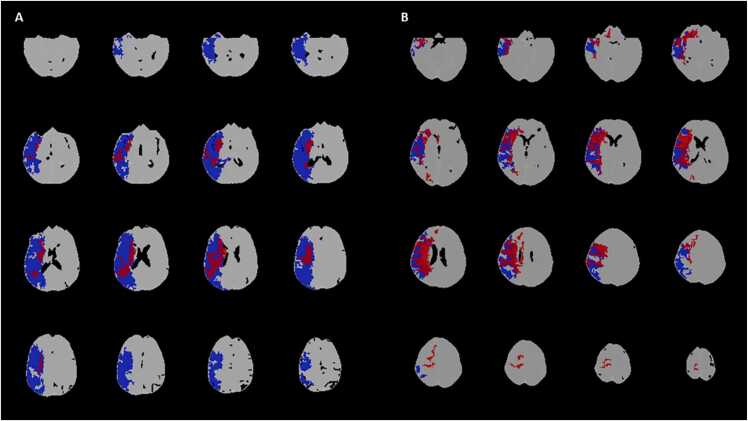
The purpose of this is study was to review pearls and pitfalls of advanced imaging, such as computed tomography perfusion and diffusion-weighed imaging and perfusion-weighted imaging in the selection of acute ischemic stroke (AIS) patients suitable for endovascular treatment (EVT) in the late time window (6-24 h from symptom onset). Advanced imaging can quantify infarct core and ischemic penumbra using specific threshold values and provides optimal selection parameters, collectively called target mismatch. More precisely, target mismatch criteria consist of core volume and/or penumbra volume and mismatch ratio (the ratio between total hypoperfusion and core volumes) with precise cut-off values. The parameters of target mismatch are automatically calculated with dedicated software packages that allow a quick and standardized interpretation of advanced imaging. However, this approach has several limitations leading to a misclassification of core and penumbra volumes. In fact, automatic software platforms are affected by technical artifacts and are not interchangeable due to a remarkable vendor-dependent variability, resulting in different estimate of target mismatch parameters. In addition, advanced imaging is not completely accurate in detecting infarct core, that can be under- or overestimated. Finally, the selection of candidates for EVT remains currently suboptimal due to the high rates of futile reperfusion and overselection caused by the use of very stringent inclusion criteria. For these reasons, some investigators recently proposed to replace advanced with conventional imaging in the selection for EVT, after the demonstration that non-contrast CT ASPECTS and computed tomography angiography collateral evaluation are not inferior to advanced images in predicting outcome in AIS patients treated with EVT. However, other authors confirmed that CTP and PWI/DWI postprocessed images are superior to conventional imaging in establishing the eligibility of patients for EVT. Therefore, the routine application of automatic assessment of advanced imaging remains a matter of debate. Recent findings suggest that the combination of conventional and advanced imaging might improving our selection criteria.
Keywords: Advanced imaging; Automatic software (maximum 6); Patient selection; Reperfusion therapies; Stroke.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Campbell B.C.V., Khatri P. Stroke. Lancet. 2020;396:129–142. - PubMed
-
- Powers W.J. Acute ischemic stroke. N. Engl. J. Med. 2020;383:252–260. - PubMed
-
- Ermine C.M., Bivard A., Parsons M.W., Baron J.C. The ischemic penumbra: from concept to reality. Int. J. Stroke. 2021;16:497–509. - PubMed
-
- Baron J.C. Protecting the ischaemic penumbra as an adjunct to thrombectomy for acute stroke. Nat. Rev. Neurol. 2018;14:325–337. - PubMed
-
- Heiss W.-D., Zaro-Weber O. Extension of therapeutic window in ischemic stroke by selective mismatch imaging. Int. J. Stroke. 2019;14:351–358. - PubMed
LinkOut - more resources
Full Text Sources
