

Compensated liver cirrhosis: Natural course and disease-modifying strategies
- PMID: 37771878
- PMCID: PMC10523240
- DOI: 10.5662/wjm.v13.i4.179
Compensated liver cirrhosis: Natural course and disease-modifying strategies
Abstract
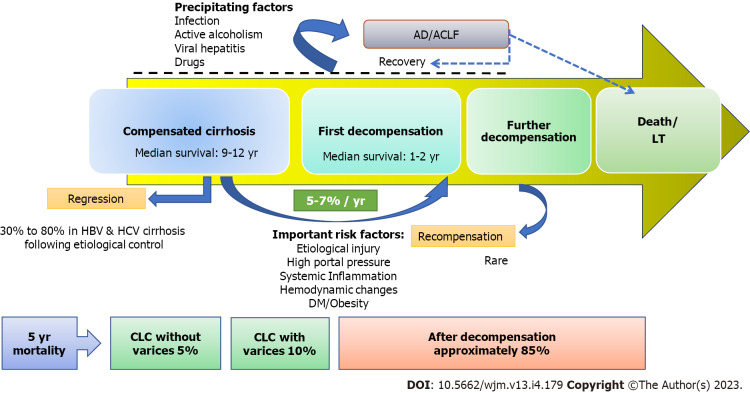
Compensated liver cirrhosis (CLC) is defined as cirrhosis with one or more decompensating events, such as ascites, variceal haemorrhage, or hepatic encephalopathy. Patients with CLC are largely asymptomatic with preserved hepatic function. The transition from CLC to decompensated cirrhosis occurs as a result of a complex interaction between multiple predisposing and precipitating factors. The first decompensation event in CLC patients is considered a significant turning point in the progression of cirrhosis, as it signals a drastic decline in median survival rates from 10-12 years to only 1-2 years. Furthermore, early cirrhosis has the potential to regress as liver fibrosis is a dynamic condition. With the advent of effective non-invasive tools for detecting hepatic fibrosis, more and more patients with CLC are currently being recognised. This offers clinicians a unique opportunity to properly manage such patients in order to achieve cirrhosis regression or, at the very least, prevent its progression. There are numerous emerging approaches for preventing or delaying decompensation in CLC patients. A growing body of evidence indicates that treating the underlying cause can lead to cirrhosis regression, and the use of non-selective beta-blockers can prevent decompensation by lowering portal hypertension. Additionally, addressing various cofactors (such as obesity, diabetes, dyslipidaemia, and alcoholism) and precipitating factors (such as infection, viral hepatitis, and hepatotoxic drugs) that have a detrimental impact on the natural course of cirrhosis may benefit patients with CLC. However, high-quality data must be generated through well-designed and adequately powered randomised clinical trials to validate these disease-modifying techniques for CLC patients. This article discussed the natural history of CLC, risk factors for its progression, and therapeutic approaches that could alter the trajectory of CLC evolution and improve outcomes.
Keywords: Acute-on-chronic liver failure; Cirrhosis reversal; Clinical decompensation; Compensated advanced chronic liver disease; Compensated cirrhosis; Disease-modifying agents.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest for this article.
Figures
Similar articles
-
Bacterial infections adversely influence the risk of decompensation and survival in compensated cirrhosis.J Hepatol. 2021 Sep;75(3):589-599. doi: 10.1016/j.jhep.2021.04.022. Epub 2021 Apr 24. J Hepatol. 2021. PMID: 33905794 Clinical Trial.
-
Transition to decompensation and acute-on-chronic liver failure: Role of predisposing factors and precipitating events.J Hepatol. 2021 Jul;75 Suppl 1:S36-S48. doi: 10.1016/j.jhep.2020.12.005. J Hepatol. 2021. PMID: 34039491 Review.
-
Presentation and complications associated with cirrhosis of the liver.Curr Med Res Opin. 2015 May;31(5):925-37. doi: 10.1185/03007995.2015.1021905. Curr Med Res Opin. 2015. PMID: 25697811 Review.
-
Short-term hemodynamic effects of β-blockers influence survival of patients with decompensated cirrhosis.J Hepatol. 2020 Oct;73(4):829-841. doi: 10.1016/j.jhep.2020.03.048. Epub 2020 Apr 13. J Hepatol. 2020. PMID: 32298768
-
New concepts on the clinical course and stratification of compensated and decompensated cirrhosis.Hepatol Int. 2018 Feb;12(Suppl 1):34-43. doi: 10.1007/s12072-017-9808-z. Epub 2017 Jul 5. Hepatol Int. 2018. PMID: 28681347 Review.
Cited by
-
Natural History of Metabolic Dysfunction-Associated Steatotic Liver Disease: From Metabolic Syndrome to Hepatocellular Carcinoma.Medicina (Kaunas). 2025 Jan 7;61(1):88. doi: 10.3390/medicina61010088. Medicina (Kaunas). 2025. PMID: 39859069 Free PMC article. Review.
-
Estimating the clinical and healthcare burden of metabolic dysfunction-associated steatohepatitis in England: a retrospective cohort study using routinely collected healthcare data from 2011 to 2020.BMJ Open. 2025 Apr 23;15(4):e095761. doi: 10.1136/bmjopen-2024-095761. BMJ Open. 2025. PMID: 40268491 Free PMC article.
-
Hepatogenous Diabetes as Compared to Type-2 Diabetes Mellitus and Non-diabetes in Patients With Liver Cirrhosis: Magnitude, Characteristics, and Implications.J Clin Exp Hepatol. 2024 Sep-Oct;14(5):101411. doi: 10.1016/j.jceh.2024.101411. Epub 2024 Apr 9. J Clin Exp Hepatol. 2024. PMID: 38699514
-
Hepatic cirrhosis and decompensation: Key indicators for predicting mortality risk.World J Hepatol. 2025 Mar 27;17(3):104580. doi: 10.4254/wjh.v17.i3.104580. World J Hepatol. 2025. PMID: 40177206 Free PMC article. Review.
-
Optimising wound care for patients with cirrhosis: A study of the effect of combination therapy on wound healing.Int Wound J. 2024 Feb;21(2):e14727. doi: 10.1111/iwj.14727. Int Wound J. 2024. Retraction in: Int Wound J. 2025 Apr;22(4):e70533. doi: 10.1111/iwj.70533. PMID: 38356305 Free PMC article. Retracted.
References
-
- Allen AM, Kim WR, Moriarty JP, Shah ND, Larson JJ, Kamath PS. Time trends in the health care burden and mortality of acute on chronic liver failure in the United States. Hepatology. 2016;64:2165–2172. - PubMed
-
- D'Amico G, Pasta L, Morabito A, D'Amico M, Caltagirone M, Malizia G, Tinè F, Giannuoli G, Traina M, Vizzini G, Politi F, Luca A, Virdone R, Licata A, Pagliaro L. Competing risks and prognostic stages of cirrhosis: a 25-year inception cohort study of 494 patients. Aliment Pharmacol Ther. 2014;39:1180–1193. - PubMed
-
- Garcia-Tsao G. Natural History of Cirrhosis. In: Keaveny A, Cárdenas A. editors. Complications of Cirrhosis. Cham Springer, 2015.
-
- D'Amico G, Bernardi M, Angeli P. Towards a new definition of decompensated cirrhosis. J Hepatol. 2022;76:202–207. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
