

Gastroesophageal junction adenocarcinoma 1-year after sleeve gastrectomy
- PMID: 37771883
- PMCID: PMC10532088
- DOI: 10.1093/jscr/rjad518
Gastroesophageal junction adenocarcinoma 1-year after sleeve gastrectomy
Abstract
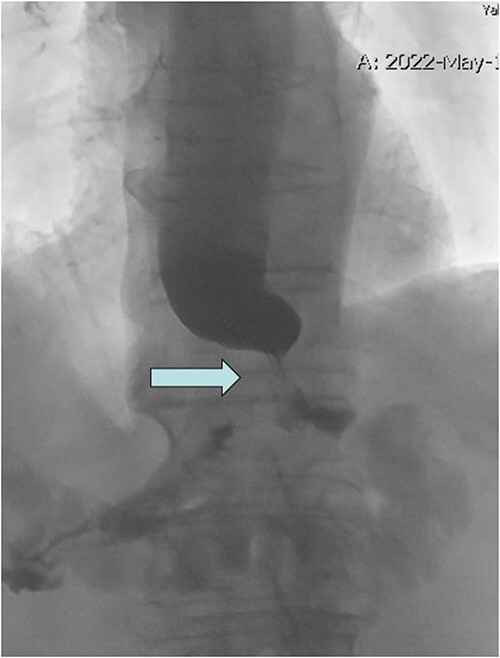
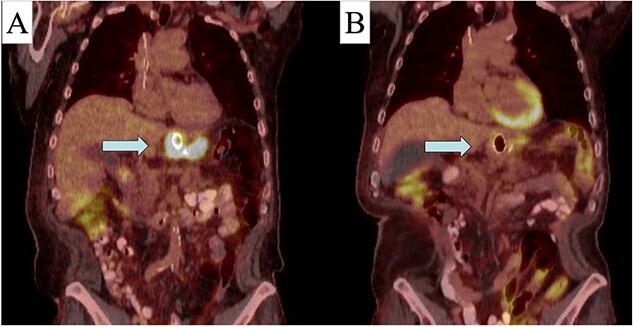
Gastroesophageal malignancy after sleeve gastrectomy is rare. A 70-year-old male with a BMI of 46 underwent laparoscopic sleeve gastrectomy with normal endoscopy. By 10 months postop, the patient had reduced BMI to 30.5. Eleven months postop, he presented with emesis and endoscopy showed severe stenosis at the gastroesophageal junction with EUS showing a circumferential mass. Patient had adenocarcinoma of the distal esophagus HER 3+ and MMR proficient, clinical T2N1. He underwent esophageal stent placement followed by FOLFOX switched to carboplatin-Taxol with radiation therapy complicated by a localized perforation requiring antibiotics. After PET scan of esophageal mass indicated response, he underwent an open distal esophagectomy, total gastrectomy with Roux-en-Y esophagojejunostomy, and placement of feeding tube. Pathology revealed poorly differentiated invasive adenocarcinoma with negative margins. In the USA, this represents only the second adenocarcinoma following a sleeve gastrectomy and the first in a non-immune compromised patient.
Keywords: cancer; endoscopy; sleeve gastrectomy.
Published by Oxford University Press and JSCR Publishing Ltd. © The Author(s) 2023.
Conflict of interest statement
None declared.
Figures

References
-
- Worldwide Obesity Federation . Prevalence of Obesity. 2023. https://www.worldobesity.org/ (September 2023, date last accessed).
-
- Anand G, Katz PO. Gastroesophageal reflux disease and obesity. Gastroenterol Clin North Am 2010;39:39–46. - PubMed
-
- Renehan AG, Tyson M, Egger M. et al. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 2008;371:569–78. - PubMed
-
- Scozzari G, Trapani R, Toppino M. et al. Esophagogastric cancer after bariatric surgery: systematic review of the literature. Surg Obes Relat Dis 2013;9:133–42. - PubMed
-
- Adams TD, Gress RE, Smith SC. et al. Long-term mortality after gastric bypass surgery. N Engl J Med 2007;357:753–61. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
