

Coronary Atherosclerosis Across the Glycemic Spectrum Among Asymptomatic Adults: The Miami Heart Study at Baptist Health South Florida
- PMID: 37772409
- PMCID: PMC10695004
- DOI: 10.1161/CIRCIMAGING.123.015314
Coronary Atherosclerosis Across the Glycemic Spectrum Among Asymptomatic Adults: The Miami Heart Study at Baptist Health South Florida
Abstract
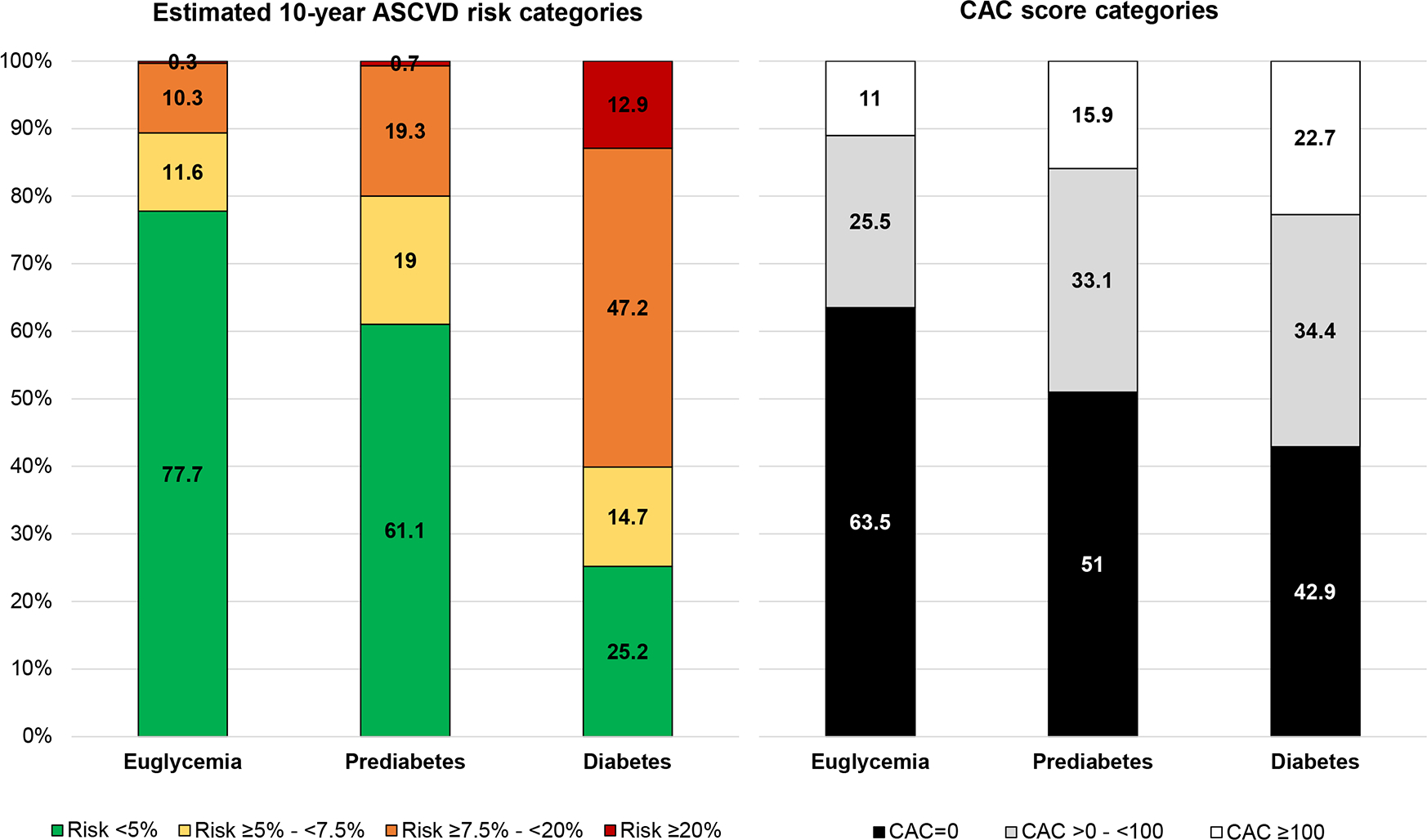
Background: The contemporary burden and characteristics of coronary atherosclerosis, assessed using coronary computed tomography angiography (CCTA), is unknown among asymptomatic adults with diabetes and prediabetes in the United States. The pooled cohort equations and coronary artery calcium (CAC) score stratify atherosclerotic cardiovascular disease risk, but their association with CCTA findings across glycemic categories is not well established.
Methods: Asymptomatic adults without atherosclerotic cardiovascular disease enrolled in the Miami Heart Study were included. Participants underwent CAC and CCTA testing and were classified into glycemic categories. Prevalence of coronary atherosclerosis (any plaque, noncalcified plaque, plaque with ≥1 high-risk feature, maximal stenosis ≥50%) assessed by CCTA was described across glycemic categories and further stratified by pooled cohort equations-estimated atherosclerotic cardiovascular disease risk and CAC score. Adjusted logistic regression was used to evaluate the associations between glycemic categories and coronary outcomes.
Results: Among 2352 participants (49.5% women), the prevalence of euglycemia, prediabetes, and diabetes was 63%, 30%, and 7%, respectively. Coronary plaque was more commonly present across worsening glycemic categories (euglycemia, 43%; prediabetes, 58%; diabetes, 69%), and similar pattern was observed for other coronary outcomes. In adjusted analyses, compared with euglycemia, prediabetes and diabetes were each associated with higher odds of any coronary plaque (OR, 1.30 [95% CI, 1.05-1.60] and 1.75 [1.17-2.61], respectively), noncalcified plaque (OR, 1.47 [1.19-1.81] and 1.99 [1.38-2.87], respectively), and plaque with ≥1 high-risk feature (OR, 1.65 [1.14-2.39] and 2.53 [1.48-4.33], respectively). Diabetes was associated with stenosis ≥50% (OR, 3.01 [1.79-5.08]; reference=euglycemia). Among participants with diabetes and estimated atherosclerotic cardiovascular disease risk <5%, 46% had coronary plaque and 10% had stenosis ≥50%. Among participants with diabetes and CAC=0, 30% had coronary plaque and 3% had stenosis ≥50%.
Conclusions: Among asymptomatic adults, worse glycemic status is associated with higher prevalence and extent of coronary atherosclerosis, high-risk plaque, and stenosis. In diabetes, CAC was more closely associated with CCTA findings and informative in a larger population than the pooled cohort equations.
Keywords: atherosclerosis; diabetes; glucose; prediabetic state; prevalence.
Conflict of interest statement
Figures


Comment in
-
Routine Coronary Atherosclerosis Imaging in the Cardiovascular Risk Assessment of Prediabetes and Diabetes.Circ Cardiovasc Imaging. 2023 Oct;16(10):e016079. doi: 10.1161/CIRCIMAGING.123.016079. Epub 2023 Sep 29. Circ Cardiovasc Imaging. 2023. PMID: 37772410 No abstract available.
References
-
- Centers for Disease Control and Prevention. National Diabetes Statistics Report website. https://www.cdc.gov/diabetes/data/statistics-report/index.html. Accessed 08/29/2022.
-
- Cainzos-Achirica M, Patel KV, Quispe R, Joshi PH, Khera A, Ayers C, Lima JAC, Rana JS, Greenland P, Bittencourt MS, et al. Coronary Artery Calcium for the Allocation of GLP-1RA for Primary Prevention of Atherosclerotic Cardiovascular Disease. JACC Cardiovasc Imaging. 2021;14:1470–1472. - PubMed
-
- Motoyama S, Ito H, Sarai M, Kondo T, Kawai H, Nagahara Y, Harigaya H, Kan S, Anno H, Takahashi H, et al. Plaque Characterization by Coronary Computed Tomography Angiography and the Likelihood of Acute Coronary Events in Mid-Term Follow-Up. J Am Coll Cardiol. 2015;66:337–46. - PubMed
