

Plasma tumour necrosis factor-alpha-related proteins in prognosis of heart failure with pulmonary hypertension
- PMID: 37772417
- PMCID: PMC10682849
- DOI: 10.1002/ehf2.14507
Plasma tumour necrosis factor-alpha-related proteins in prognosis of heart failure with pulmonary hypertension
Abstract
Aims: Patients with heart failure (HF) exhibit poor prognosis, which is further deteriorated by pulmonary hypertension (PH), with negative impact on morbidity and mortality. As PH due to left HF (LHF-PH) is among the most common causes of PH, there is an urge according to the 2021 European Society of Cardiology HF guidelines to find new biomarkers that aid in prognostication of this patient cohort. Given the role of tumour necrosis factor-alpha (TNF-α) in HF progression, we aimed to investigate the prognostic value of plasma proteins related to TNF-α in patients with LHF-PH, in relation to haemodynamic changes following heart transplantation (HT).
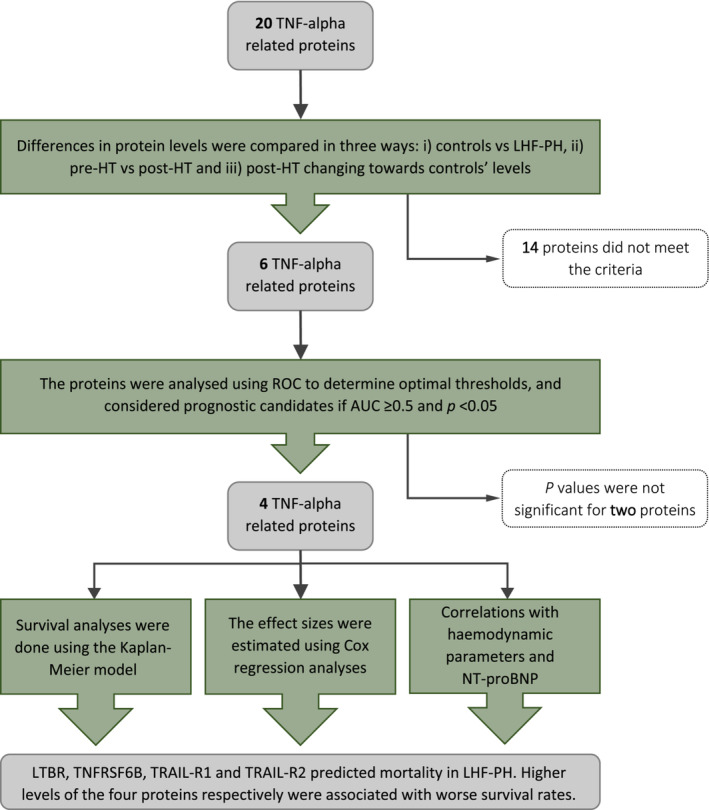
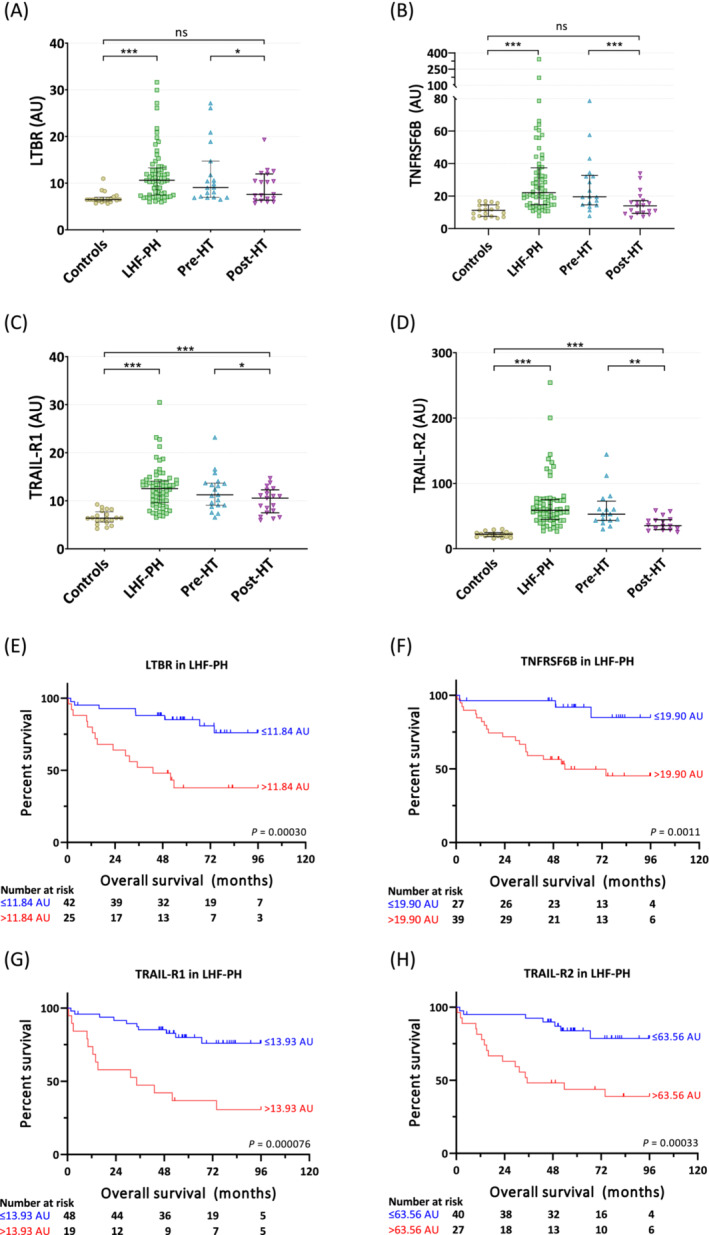
Methods and results: Twenty TNF-α-related plasma proteins were analysed using proximity extension assay in healthy controls (n = 20) and patients with LHF-PH (n = 67), before and 1 year after HT (n = 19). Plasma levels were compared between the groups, and the prognostic values were determined using Kaplan-Meier and Cox regression analyses. Plasma levels of lymphotoxin-beta receptor (LTBR), TNF receptor superfamily member 6B (TNFRSF6B), and TNF-related apoptosis-inducing ligand receptors 1 and 2 (TRAIL-R1 and TRAIL-R2, respectively) were higher in LHF-PH pre-HT vs. controls (P < 0.0001), as well as higher in pre-HT vs. post-HT (P < 0.001). The elevated pre-HT levels of LTBR, TNFRSF6B, TRAIL-R1, and TRAIL-R2 decreased towards the levels of healthy controls after HT. Higher preoperative levels of LTBR, TNFRSF6B, TRAIL-R1, and TRAIL-R2 in LHF-PH were associated with worse survival rates (P < 0.002). In multivariate Cox regression models, each adjusted for age and sex, LTBR, TNFRSF6B, TRAIL-R1, and TRAIL-R2 predicted mortality (P < 0.002) [hazard ratio (95% confidence interval): 1.12 (1.04-1.19), 1.01 (1.004-1.02), 1.28 (1.14-1.42), and 1.03 (1.02-1.04), respectively].
Conclusions: Elevated pre-HT plasma levels of the TNF-α-related proteins LTBR, TNFRSF6B, TRAIL-R1, and TRAIL-R2 in LHF-PH decreased 1 year after HT, displaying a normalization pattern towards the levels of the healthy controls. These proteins were also prognostic, where higher levels were associated with worse survival rates in LHF-PH, providing new insight in their potential role as prognostic biomarkers. Larger studies are warranted to validate our findings and to investigate their possible pathobiological mechanisms in LHF-PH.
Keywords: Biomarkers; Cardiovascular diseases; Haemodynamics; Multi-marker panel; Pulmonary hypertension; Survival.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
A.E. and S.H. report no relationships that could be construed as a conflict of interest. A.A. and S.A. report personal lecture fees from Janssen‐Cilag AB outside the submitted work. G.R. reports personal lecture fees from Actelion Pharmaceuticals Sweden AB, GlaxoSmithKline, Bayer Health Care, Janssen, and Nordic Infucare outside the submitted work; reports unrestricted research grants from ALF and Janssen during the conduct of the study; and is, and has been, primary, or co‐, investigator in clinical PAH trials for Acceleron, Actelion Pharmaceuticals Sweden AB, GlaxoSmithKline, Janssen, Pfizer, Bayer, and United Therapeutics and in clinical heart transplantation immunosuppression trials for Novartis. The companies had no role in the data collection, analysis, and interpretation and had no right in disapproving of the manuscript.
Figures
Similar articles
-
Elevated plasma WIF-1 levels are associated with worse prognosis in heart failure with pulmonary hypertension.ESC Heart Fail. 2022 Dec;9(6):4139-4149. doi: 10.1002/ehf2.14148. Epub 2022 Sep 9. ESC Heart Fail. 2022. PMID: 36082780 Free PMC article.
-
Adrenomedullin peptides and precursor levels in relation to haemodynamics and prognosis after heart transplantation.ESC Heart Fail. 2023 Aug;10(4):2427-2437. doi: 10.1002/ehf2.14399. Epub 2023 May 28. ESC Heart Fail. 2023. PMID: 37246315 Free PMC article.
-
Higher plasma IL-6 and PTX3 are associated with worse survival in left heart failure with pulmonary hypertension.Am Heart J Plus. 2022 Aug 10;20:100190. doi: 10.1016/j.ahjo.2022.100190. eCollection 2022 Aug. Am Heart J Plus. 2022. PMID: 38560419 Free PMC article.
-
Plasma tumour and metabolism related biomarkers AMBP, LPL and Glyoxalase I differentiate heart failure with preserved ejection fraction with pulmonary hypertension from pulmonary arterial hypertension.Int J Cardiol. 2021 Dec 15;345:68-76. doi: 10.1016/j.ijcard.2021.10.136. Epub 2021 Oct 25. Int J Cardiol. 2021. PMID: 34710494
-
TRAIL or TRAIL-R2 as a Predictive Biomarker for Mortality or Cardiovascular Events: A Systematic Review and Meta-analysis.J Cardiovasc Pharmacol. 2023 May 1;81(5):348-354. doi: 10.1097/FJC.0000000000001415. J Cardiovasc Pharmacol. 2023. PMID: 36888983
Cited by
-
Biomarkers in heart failure: Traditional and emerging indicators for prognosis.ESC Heart Fail. 2025 Jun;12(3):1535-1538. doi: 10.1002/ehf2.15168. Epub 2024 Nov 15. ESC Heart Fail. 2025. PMID: 39545304 Free PMC article. No abstract available.
-
Apoptosis in Cardiac Conditions Including Cirrhotic Cardiomyopathy.Int J Mol Sci. 2025 Jul 3;26(13):6423. doi: 10.3390/ijms26136423. Int J Mol Sci. 2025. PMID: 40650199 Free PMC article. Review.
-
Hepatocyte Growth Factor: A Marker of Cardiac Function, Mortality, and Disease Subtype in Cardiac Amyloidosis.JACC Adv. 2025 May 30;4(6 Pt 1):101828. doi: 10.1016/j.jacadv.2025.101828. Online ahead of print. JACC Adv. 2025. PMID: 40570404 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
