

Therapeutic S100A8/A9 blockade inhibits myocardial and systemic inflammation and mitigates sepsis-induced myocardial dysfunction
- PMID: 37773186
- PMCID: PMC10540409
- DOI: 10.1186/s13054-023-04652-x
Therapeutic S100A8/A9 blockade inhibits myocardial and systemic inflammation and mitigates sepsis-induced myocardial dysfunction
Abstract
Background and aims: The triggering factors of sepsis-induced myocardial dysfunction (SIMD) are poorly understood and are not addressed by current treatments. S100A8/A9 is a pro-inflammatory alarmin abundantly secreted by activated neutrophils during infection and inflammation. We investigated the efficacy of S100A8/A9 blockade as a potential new treatment in SIMD.
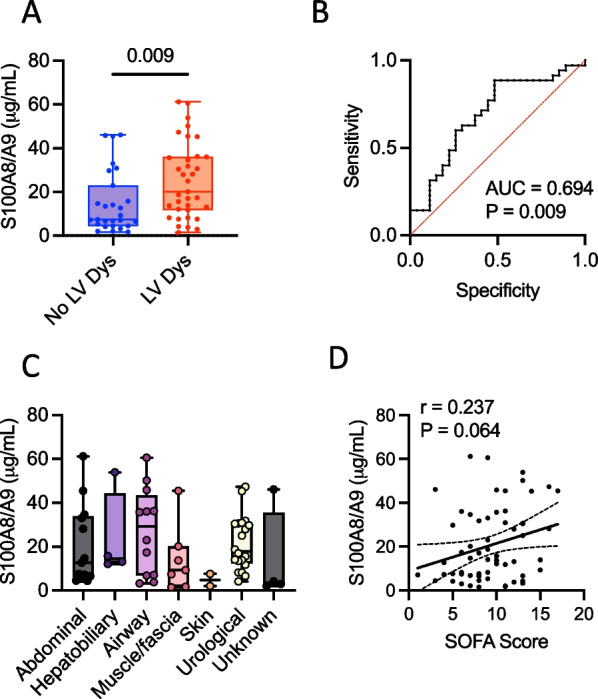
Methods: The relationship between plasma S100A8/A9 and cardiac dysfunction was assessed in a cohort of 62 patients with severe sepsis admitted to the intensive care unit of Linköping University Hospital, Sweden. We used S100A8/A9 blockade with the small-molecule inhibitor ABR-238901 and S100A9-/- mice for therapeutic and mechanistic studies on endotoxemia-induced cardiac dysfunction in mice.
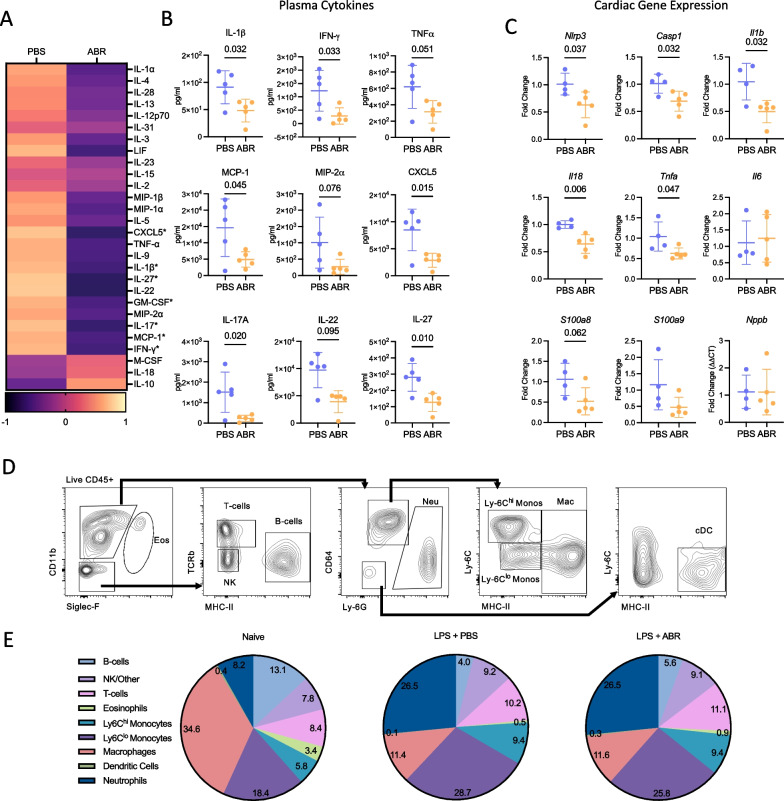
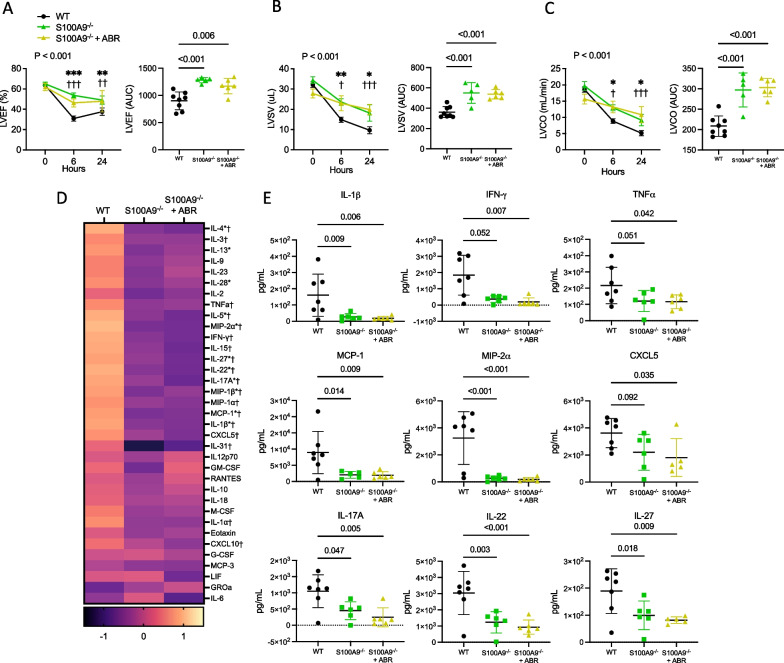
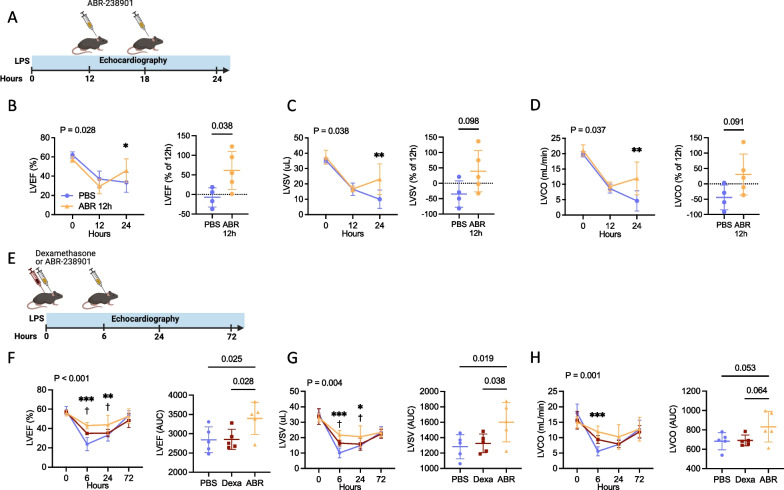
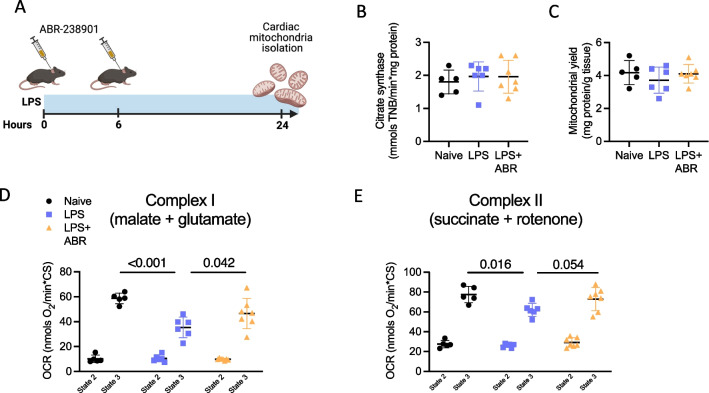
Results: In sepsis patients, elevated plasma S100A8/A9 was associated with left-ventricular (LV) systolic dysfunction and increased SOFA score. In wild-type mice, 5 mg/kg of bacterial lipopolysaccharide (LPS) induced rapid plasma S100A8/A9 increase and acute LV dysfunction. Two ABR-238901 doses (30 mg/kg) administered intraperitoneally with a 6 h interval, starting directly after LPS or at a later time-point when LV dysfunction is fully established, efficiently prevented and reversed the phenotype, respectively. In contrast, dexamethasone did not improve cardiac function compared to PBS-treated endotoxemic controls. S100A8/A9 inhibition potently reduced systemic levels of inflammatory mediators, prevented upregulation of inflammatory genes and restored mitochondrial function in the myocardium. The S100A9-/- mice were protected against LPS-induced LV dysfunction to an extent comparable with pharmacologic S100A8/A9 blockade. The ABR-238901 treatment did not induce an additional improvement of LV function in the S100A9-/- mice, confirming target specificity.
Conclusion: Elevated S100A8/A9 is associated with the development of LV dysfunction in severe sepsis patients and in a mouse model of endotoxemia. Pharmacological blockade of S100A8/A9 with ABR-238901 has potent anti-inflammatory effects, mitigates myocardial dysfunction and might represent a novel therapeutic strategy for patients with severe sepsis.
Keywords: Endotoxemia; Inflammation; Mitochondrial function; Neutrophils; S100A8/A9; Sepsis-induced myocardial dysfunction.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
Michelle Chew is a member of the editorial board of Critical Care.
Figures

Comment in
-
Potential confounders in linking elevated S100A8/A9 to left ventricular dysfunction in septic shock patients.Crit Care. 2023 Dec 6;27(1):480. doi: 10.1186/s13054-023-04769-z. Crit Care. 2023. PMID: 38057840 Free PMC article. No abstract available.
-
Reply to "Potential confounders in linking elevated S100A8/A9 to left ventricular dysfunction in septic shock patients".Crit Care. 2024 Jan 2;28(1):9. doi: 10.1186/s13054-023-04789-9. Crit Care. 2024. PMID: 38167162 Free PMC article. No abstract available.
References
-
- Gotts JE, Matthay MA. Sepsis: pathophysiology and clinical management. BMJ. 2016;353:i1585. - PubMed
-
- Angus DC, van der Poll T. Severe sepsis and septic shock. New Engl J Med. 2013;369:840–851. - PubMed
-
- Beesley SJ, Weber G, Sarge T, Nikravan S, Grissom CK, Lanspa MJ, et al. Septic cardiomyopathy. Crit Care Med. 2018;46:625–634. - PubMed
-
- Calvin JE, Driedger AA, Sibbald WJ. An assessment of myocardial function in human sepsis utilizing ECG gated cardiac scintigraphy. Chest. 1981;80:579–586. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
