

Choroidal morphology and microvascular structure in eyes of patients with idiopathic normal pressure hydrocephalus before and after ventriculo-peritoneal shunt surgery
- PMID: 37773320
- PMCID: PMC10541413
- DOI: 10.1038/s41598-023-43518-8
Choroidal morphology and microvascular structure in eyes of patients with idiopathic normal pressure hydrocephalus before and after ventriculo-peritoneal shunt surgery
Abstract
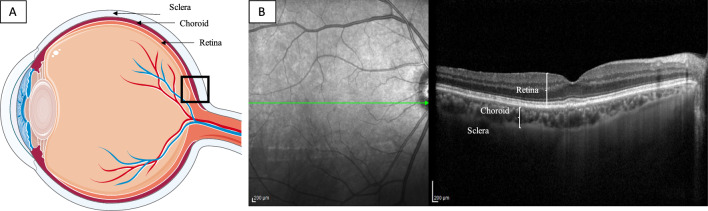
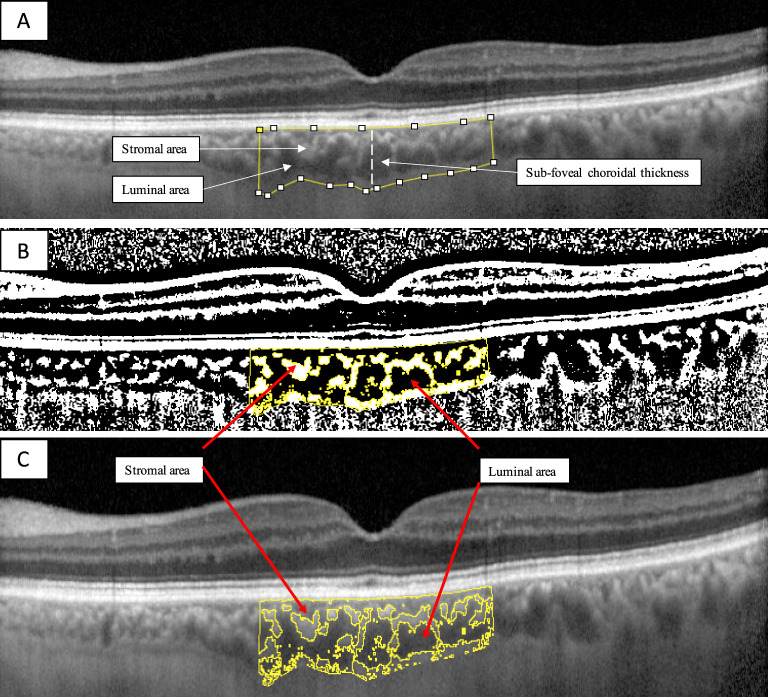
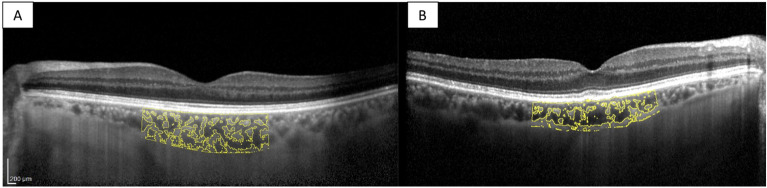
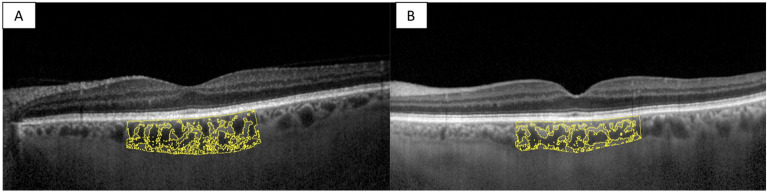
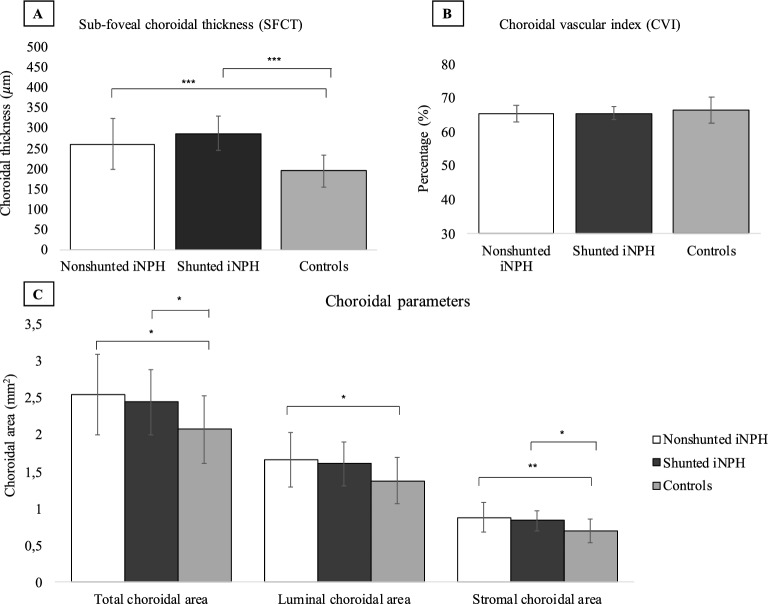
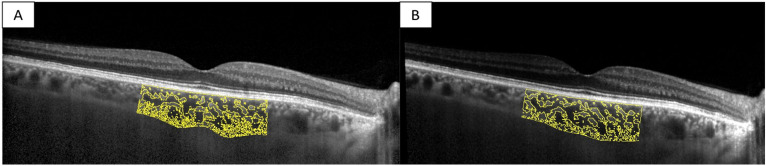
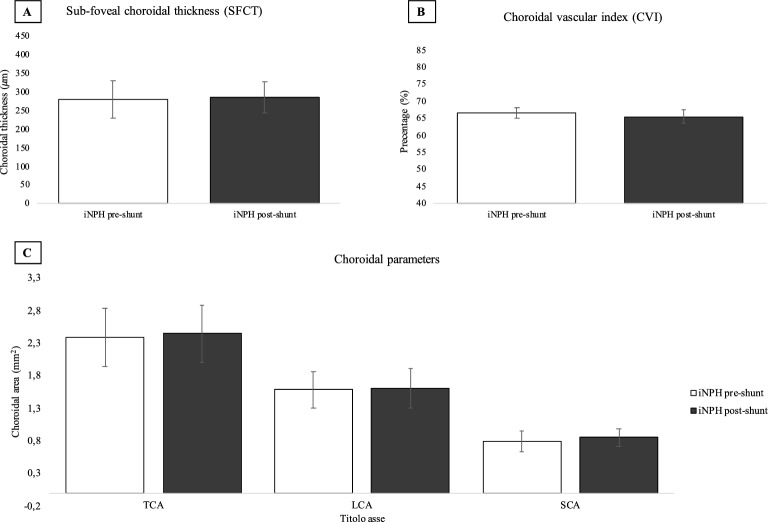
The present study aims to investigate the choroidal morphology and microvascular structure in eyes of patients with idiopathic normal pressure hydrocephalus (iNPH) compared with the eyes of healthy age-matched individuals, and to assess the choroidal structure in eyes of iNPH patients before and after shunt surgery using Optical Coherence Tomography (OCT). The primary objective was to assess the choroidal morphology in eyes of iNPH patients before and after ventriculo-peritoneal (VP) surgery compared to age and sex-matched healthy individuals. The secondary objective was to compare the choroidal morphology of iNPH patients before and after a mean of 56 days from shunt surgery. Eighteen consecutive patients diagnosed with iNPH and 18 healthy controls were prospectively recruited between November 2021 and October 2022. Spectral-domain optical coherence tomography (SD-OCT) with enhanced depth imaging (EDI) was conducted before and within 4 months after shunt surgery. Images were binarized using the ImageJ software, and the choroidal vascular index (CVI) was calculated. Sub-foveal choroidal thickness (SFCT), total choroidal area (TCA), luminal choroidal area (LCA), and stromal choroidal area (SCA) were significantly increased in iNPH patients before surgery compared to the control group (p < 0.05). SFCT, TCA, and SCA were significantly increased in iNPH patients after surgery compared to the control group (p < 0.05). There were no differences in the CVI between iNPH patients and controls. No statistical differences in the choroidal structure were observed before and after VP shunt surgery (p > 0.05). In conclusion, the choroid was thicker in iNPH patients before and after VP shunt compared to age-matched healthy individuals. However, there were no difference in the choroidal microstructure in the eyes of iNPH patients before and after a mean of 3 months from VP shunt surgery.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Shaw R, Everingham E, Mahant N, Jacobson E, Owler B. Clinical outcomes in the surgical treatment of idiopathic normal pressure hydrocephalus. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2016;29:81–86. - PubMed
-
- Giordan E, Palandri G, Lanzino G, Murad MH, Elder BD. Outcomes and complications of different surgical treatments for idiopathic normal pressure hydrocephalus: A systematic review and meta-analysis. J. Neurosurg. 2018;1:1–13. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
