

Evaluation of Predict, a prognostic risk tool, after diagnosis of a second breast cancer
- PMID: 37773987
- PMCID: PMC10660126
- DOI: 10.1093/jncics/pkad081
Evaluation of Predict, a prognostic risk tool, after diagnosis of a second breast cancer
Abstract
Background: The UK National Health Service's Predict is a clinical tool widely used to estimate the prognosis of early-stage breast cancer. The performance of Predict for a second primary breast cancer is unknown.
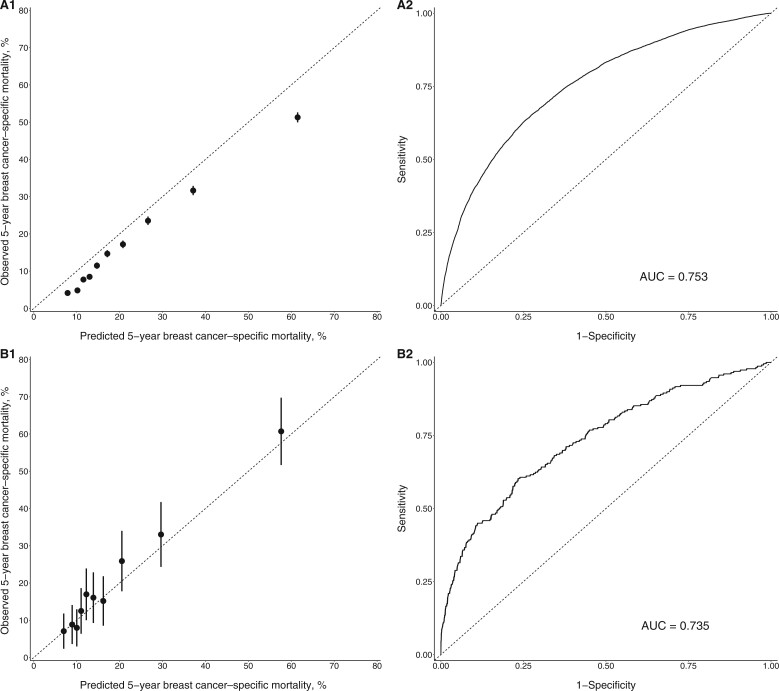
Methods: Women 18 years of age or older diagnosed with a first or second invasive breast cancer between 2000 and 2013 and followed for at least 5 years were identified from the US Surveillance, Epidemiology, and End Results (SEER) database. Model calibration of Predict was evaluated by comparing predicted and observed 5-year breast cancer-specific mortality separately by estrogen receptor status for first vs second breast cancer. Receiver operating characteristic curves and areas under the curve were used to assess model discrimination. Model performance was also evaluated for various races and ethnicities.
Results: The study population included 6729 women diagnosed with a second breast cancer and 357 204 women with a first breast cancer. Overall, Predict demonstrated good discrimination for first and second breast cancers (areas under the curve ranging from 0.73 to 0.82). Predict statistically significantly underestimated 5-year breast cancer mortality for second estrogen receptor-positive breast cancers (predicted-observed = ‒6.24%, 95% CI = ‒6.96% to ‒5.49%). Among women with a first estrogen receptor-positive cancer, model calibration was good (predicted-observed = ‒0.22%, 95% CI = ‒0.29% to ‒0.15%), except in non-Hispanic Black women (predicted-observed = ‒2.33%, 95% CI = ‒2.65% to ‒2.01%) and women 80 years of age or older (predicted-observed = ‒3.75%, 95% CI = ‒4.12% to ‒3.41%). Predict performed well for second estrogen receptor-negative cancers overall (predicted-observed = ‒1.69%, 95% CI = ‒3.99% to 0.16%) but underestimated mortality among those who had previously received chemotherapy or had a first cancer with more aggressive tumor characteristics. In contrast, Predict overestimated mortality for first estrogen receptor-negative cancers (predicted-observed = 4.54%, 95% CI = 4.27% to 4.86%).
Conclusion: The Predict tool underestimated 5-year mortality after a second estrogen receptor-positive breast cancer and in certain subgroups of women with a second estrogen receptor-negative breast cancer.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
K.V. reports funding from Cepheid and nonfinancial support from Optra Health Inc. K.V. also holds a patent for C11625. A.C.W. reports holding a patent for C12014—A quantitative Multiplex Methylation Specific PCR Method-cMethDNA, reagents, and its use is licensed (license terminated by Cepheid, 2020).
Figures

References
-
- Curtis RE, Freedman DM, Ron E, et al. (eds). New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute, NIH Publ. No. 05-5302; 2006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical