

Interplay Between Chronic Kidney Disease, Hypertension, and Stroke: Insights From a Multivariable Mendelian Randomization Analysis
- PMID: 37775316
- PMCID: PMC10662984
- DOI: 10.1212/WNL.0000000000207852
Interplay Between Chronic Kidney Disease, Hypertension, and Stroke: Insights From a Multivariable Mendelian Randomization Analysis
Erratum in
-
Corrections to Preprint Server Information.Neurology. 2024 Jul 9;103(1):e209573. doi: 10.1212/WNL.0000000000209573. Epub 2024 Jun 3. Neurology. 2024. PMID: 38830142 Free PMC article. No abstract available.
-
Corrections to Received Date Information.Neurology. 2024 Jul 9;103(1):e209596. doi: 10.1212/WNL.0000000000209596. Epub 2024 Jun 3. Neurology. 2024. PMID: 38830175 Free PMC article. No abstract available.
Abstract
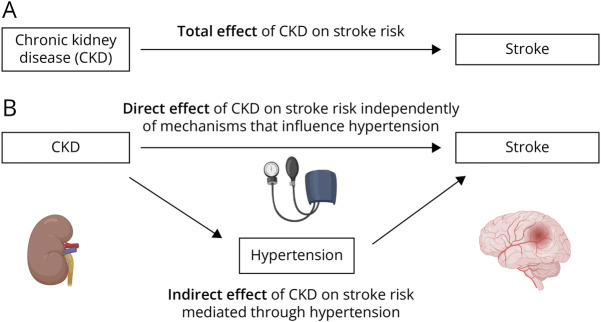
Background and objectives: Chronic kidney disease (CKD) increases the risk of stroke, but the extent through which this association is mediated by hypertension is unknown. We leveraged large-scale genetic data to explore causal relationships between CKD, hypertension, and cerebrovascular disease phenotypes.
Methods: We used data from genome-wide association studies of European ancestry to identify genetic proxies for kidney function (CKD diagnosis, estimated glomerular filtration rate [eGFR], and urinary albumin-to-creatinine ratio [UACR]), systolic blood pressure (SBP), and cerebrovascular disease (ischemic stroke and its subtypes and intracerebral hemorrhage). We then conducted univariable, multivariable, and mediation Mendelian randomization (MR) analyses to investigate the effect of kidney function on stroke risk and the proportion of this effect mediated through hypertension.
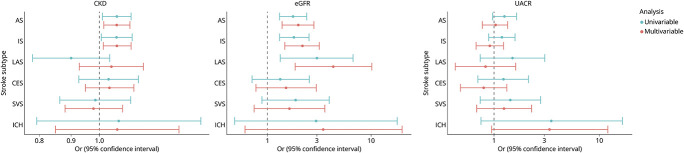
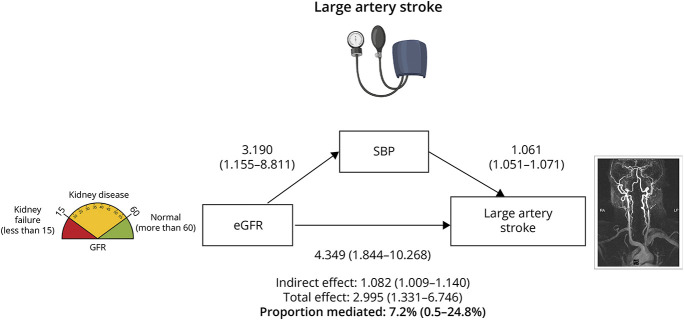
Results: Univariable MR revealed associations between genetically determined lower eGFR and risk of all stroke (odds ratio [OR] per 1-log decrement in eGFR, 1.77; 95% CI 1.31-2.40; p < 0.001), ischemic stroke (OR 1.81; 95% CI 1.31-2.51; p < 0.001), and most strongly with large artery stroke (LAS) (OR 3.00; 95% CI 1.33-6.75; p = 0.008). These associations remained significant in the multivariable MR analysis, controlling for SBP (OR 1.98; 95% CI 1.39-2.82; p < 0.001 for all stroke; OR 2.16; 95% CI 1.48-3.17; p < 0.001 for ischemic stroke; OR 4.35; 95% CI 1.84-10.27; p = 0.001 for LAS), with only a small proportion of the total effects mediated by SBP (6.5% [0.7%-16.8%], 6.6% [0.8%-18.3%], and 7.2% [0.5%-24.8%], respectively). Total, direct and indirect effect estimates were similar across a number of sensitivity analyses (weighted median, MR-Egger regression).
Discussion: Our results demonstrate an independent causal effect of impaired kidney function, as assessed by decreased eGFR, on stroke risk, particularly LAS, even when controlled for SBP. Targeted prevention of kidney disease could lower atherosclerotic stroke risk independent of hypertension.
© 2023 American Academy of Neurology.
Conflict of interest statement
D.M. Kelly is an Atlantic Fellow for Equity in Brain Health at the Global Brain Health Institute (GBHI) and is supported with funding from GBHI, Alzheimer's Association, and Alzheimer's Society (GBHI ALZ UK-22-868940) and is the recipient of an NIH StrokeNet Fellowship. M.K. Georgakis is supported by a Walter-Benjamin fellowship from the German Research Foundation (Deutsche Forschungsgemeinschaft [DFG], GZ: GE 3461/1-1) and the FöFoLe program of Ludwig-Maximilians-University Munich (FöFoLe-Forschungsprojekt Reg.-Nr. 1120). This work was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany's Excellence Strategy within the framework of the Munich Cluster for Systems Neurology (EXC 2145 SyNergy: ID 390857198 to MKG). N. Franceschini is supported by NIH R01 HL163972. A. Viswanathan is supported by NIH P50 AG005134 NIH AG047975 R01 NS104130. C.D. Anderson is supported by NIH R01NS103924, U01NS069673, AHA 18SFRN34250007, and AHA-Bugher 21SFRN812095 for this work and receives sponsored research support from Bayer AG and has consulted for ApoPharma, Inc. Go to
Figures
Similar articles
-
Genetic overlap and causal inferences between kidney function and cerebrovascular disease.Neurology. 2020 Jun 16;94(24):e2581-e2591. doi: 10.1212/WNL.0000000000009642. Epub 2020 May 21. Neurology. 2020. PMID: 32439819 Free PMC article.
-
Causal Relationship Between Kidney Function and Cancer Risk: A Mendelian Randomization Study.Am J Kidney Dis. 2024 Dec;84(6):686-695.e1. doi: 10.1053/j.ajkd.2024.05.016. Epub 2024 Jul 30. Am J Kidney Dis. 2024. PMID: 39084486
-
Causal effects of plasma metabolites on chronic kidney diseases and renal function: a bidirectional Mendelian randomization study.Front Endocrinol (Lausanne). 2024 Jul 26;15:1429159. doi: 10.3389/fendo.2024.1429159. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39129920 Free PMC article.
-
Causality of visceral adipose tissue on chronic kidney disease and renal function measure indicators, and mediation role of hypertension: Mendelian randomization study.Obes Rev. 2025 Feb;26(2):e13845. doi: 10.1111/obr.13845. Epub 2024 Oct 10. Obes Rev. 2025. PMID: 39390683 Free PMC article. Review.
-
The role of mitochondrial DNA copy number in cardiometabolic disease: a bidirectional two-sample mendelian randomization study.Cardiovasc Diabetol. 2024 Jan 28;23(1):45. doi: 10.1186/s12933-023-02074-1. Cardiovasc Diabetol. 2024. PMID: 38282013 Free PMC article. Review.
Cited by
-
Corrections to Received Date Information.Neurology. 2024 Jul 9;103(1):e209596. doi: 10.1212/WNL.0000000000209596. Epub 2024 Jun 3. Neurology. 2024. PMID: 38830175 Free PMC article. No abstract available.
-
Cardiovascular Risk and Its Presentation in Chronic Kidney Disease.J Clin Med. 2025 Jun 27;14(13):4567. doi: 10.3390/jcm14134567. J Clin Med. 2025. PMID: 40648948 Free PMC article. Review.
-
Investigating the Prevalence and Predictors of Uncontrolled Hypertension: A Cross-Sectional Study in Gujarat, India.Cureus. 2024 Apr 25;16(4):e59036. doi: 10.7759/cureus.59036. eCollection 2024 Apr. Cureus. 2024. PMID: 38800155 Free PMC article.
-
Association of Differences in Cystatin C- and Creatinine-Based Estimated Glomerular Filtration Rate With Prevalence and Incidence of Stroke.J Am Heart Assoc. 2025 Jun 3;14(11):e039185. doi: 10.1161/JAHA.124.039185. Epub 2025 May 23. J Am Heart Assoc. 2025. PMID: 40407072 Free PMC article.
-
Mendelian randomization studies of lifestyle-related risk factors for stroke: a systematic review and meta-analysis.Front Endocrinol (Lausanne). 2024 Nov 4;15:1379516. doi: 10.3389/fendo.2024.1379516. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39558973 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous