

Clinical impact of an integrated e-health system for diabetes self-management support and shared decision making (POWER2DM): a randomised controlled trial
- PMID: 37775611
- PMCID: PMC10627940
- DOI: 10.1007/s00125-023-06006-2
Clinical impact of an integrated e-health system for diabetes self-management support and shared decision making (POWER2DM): a randomised controlled trial
Abstract
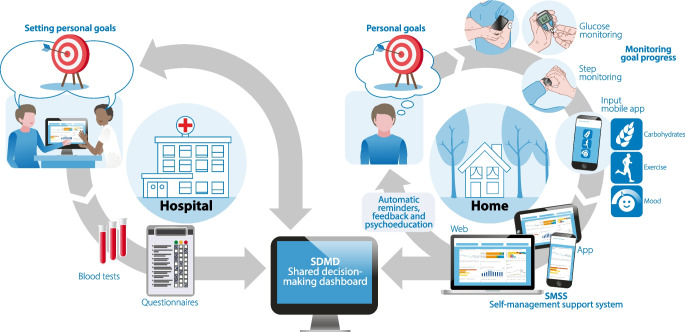
Aims/hypothesis: There is a lack of e-health systems that integrate the complex variety of aspects relevant for diabetes self-management. We developed and field-tested an e-health system (POWER2DM) that integrates medical, psychological and behavioural aspects and connected wearables to support patients and healthcare professionals in shared decision making and diabetes self-management.
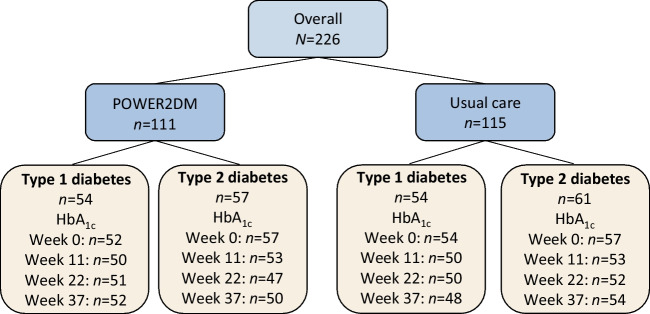
Methods: Participants with type 1 or type 2 diabetes (aged >18 years) from hospital outpatient diabetes clinics in the Netherlands and Spain were randomised using randomisation software to POWER2DM or usual care for 37 weeks. This RCT assessed the change in HbA1c between the POWER2DM and usual care groups at the end of the study (37 weeks) as a primary outcome measure. Participants and clinicians were not blinded to the intervention. Changes in quality of life (QoL) (WHO-5 Well-Being Index [WHO-5]), diabetes self-management (Diabetes Self-Management Questionnaire - Revised [DSMQ-R]), glycaemic profiles from continuous glucose monitoring devices, awareness of hypoglycaemia (Clarke hypoglycaemia unawareness instrument), incidence of hypoglycaemic episodes and technology acceptance were secondary outcome measures. Additionally, sub-analyses were performed for participants with type 1 and type 2 diabetes separately.
Results: A total of 226 participants participated in the trial (108 with type 1 diabetes; 118 with type 2 diabetes). In the POWER2DM group (n=111), HbA1c decreased from 60.6±14.7 mmol/mol (7.7±1.3%) to 56.7±12.1 mmol/mol (7.3±1.1%) (means ± SD, p<0.001), compared with no change in the usual care group (n=115) (baseline: 61.7±13.7 mmol/mol, 7.8±1.3%; end of study: 61.0±12.4 mmol/mol, 7.7±1.1%; p=0.19) (between-group difference 0.24%, p=0.008). In the sub-analyses in the POWER2DM group, HbA1c in participants with type 2 diabetes decreased from 62.3±17.3 mmol/mol (7.9±1.6%) to 54.3±11.1 mmol/mol (7.1±1.0%) (p<0.001) compared with no change in HbA1c in participants with type 1 diabetes (baseline: 58.8±11.2 mmol/mol [7.5±1.0%]; end of study: 59.2±12.7 mmol/mol [7.6±1.2%]; p=0.84). There was an increase in the time during which interstitial glucose levels were between 3.0 and 3.9 mmol/l in the POWER2DM group, but no increase in clinically relevant hypoglycaemia (interstitial glucose level below 3.0 mmol/l). QoL improved in participants with type 1 diabetes in the POWER2DM group compared with the usual care group (baseline: 15.7±3.8; end of study: 16.3±3.5; p=0.047 for between-group difference). Diabetes self-management improved in both participants with type 1 diabetes (from 7.3±1.2 to 7.7±1.2; p=0.002) and those with type 2 diabetes (from 6.5±1.3 to 6.7±1.3; p=0.003) within the POWER2DM group. The POWER2DM integrated e-health support was well accepted in daily life and no important adverse (or unexpected) effects or side effects were observed.
Conclusions/interpretation: POWER2DM improves HbA1c levels compared with usual care in those with type 2 diabetes, improves QoL in those with type 1 diabetes, improves diabetes self-management in those with type 1 and type 2 diabetes, and is well accepted in daily life.
Trial registration: ClinicalTrials.gov NCT03588104.
Funding: This study was funded by the European Union's Horizon 2020 Research and Innovation Programme (grant agreement number 689444).
Keywords: Diabetes; Glycaemic control; Quality of life; RCT; Self-management; Shared decision making; e-health; m-health.
© 2023. The Author(s).
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
