

Macrofollicular Architecture in Invasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Pitfall in Thyroid Practice
- PMID: 37775618
- PMCID: PMC10739678
- DOI: 10.1007/s12105-023-01584-4
Macrofollicular Architecture in Invasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Pitfall in Thyroid Practice
Abstract
Background: Predominantly macrofollicular architecture in invasive encapsulated follicular variant of papillary thyroid carcinoma (IEFVPTC-MF) is rare and often a cause of misinterpretation during pre-operative work-up and histopathology evaluation. We comprehensively evaluated the radiological, cytological, gross, microscopic, molecular and follow-up characteristics of four such cases, intending to increase its recognition and add our experience to the limited literature available.
Methods: All such histopathologically-proven cases of IEFVPTC-MF were retrieved from the departmental archives. The clinical details, thyroid ultrasound, cytology and thyroid scan findings were reviewed. Allele-specific PCR for BRAF p.V600E, KRAS, NRAS, and HRAS mutations, and FISH assays for ETV6::NTRK3 fusion and RET fusions were performed.
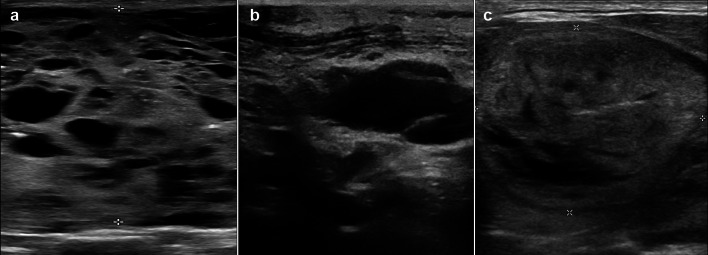
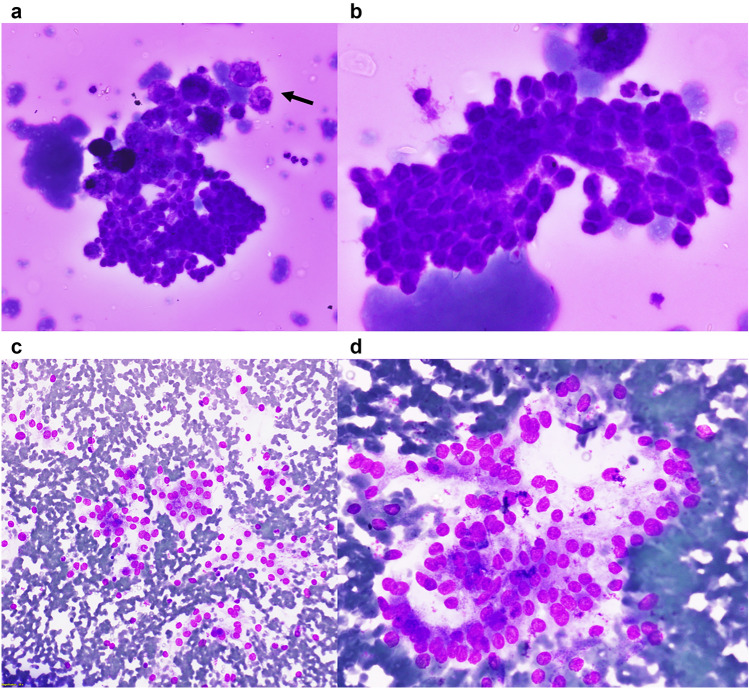
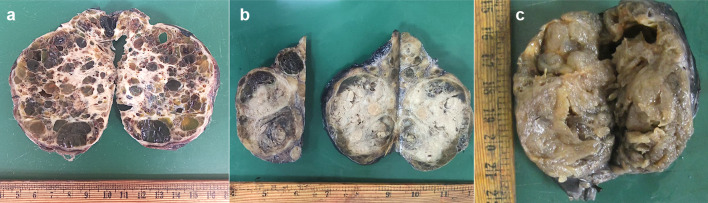
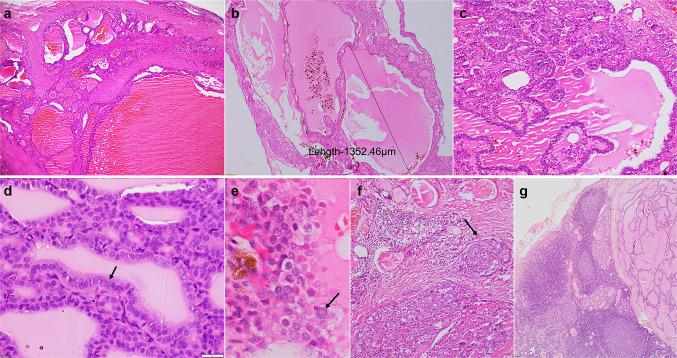
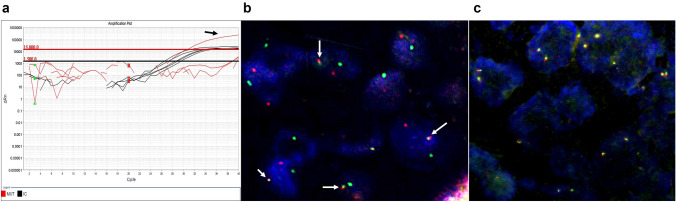
Results: There were four cases of IEFVPTC-MF diagnosed between 2021 and 2022, involving two males and two females. The median age at presentation was 27 years, and the duration of the disease was 1-10 years. Thyroid ultrasound was TR1 (benign; n = 1), TR2 (not suspicious; n = 2), or TR4 (moderately suspicious; n = 1). Cytology was categorized as nondiagnostic (n = 1), benign (n = 1), and atypia of undetermined significance (n = 1). The three nodules with available cytology smears showed abundant colloid. Cells were arranged as sheets/microfollicles/clusters. Nuclei were predominantly round with minimal/focal elongation, membrane irregularity, and cellular crowding. On gross examination, cut surfaces of the tumors showed variable amounts of colloid. The tumors were solid-cystic. Histopathology revealed partially encapsulated multinodular tumors. There were prominent pseudopapillae projecting into the lumina of macrofollicles. Nuclei were predominantly round with variable nuclear atypia, including chromatin clearing and multifocal presence of nuclear grooves. Pseudoinclusions were identified in two. Molecular analysis revealed NRAS codon 61 mutation and ETV6::NTRK3 fusion in one case each. Two patients had cervical lymph node and hematogenous metastases. Post-radio-active iodine, the response was structurally incomplete (n = 2), indeterminate (n = 1) and excellent (n = 1).
Conclusions: Macrofollicular architecture in invasive encapsulated follicular variant of papillary thyroid carcinoma is a major pitfall in thyroid oncology practice. Long-standing disease, and ultrasonographic and cytological features that overlap with benign disease, often lead to underdiagnosis during pre-operative evaluation. As patients may consequently develop distant metastases and have inadequate treatment response, there is a need for more vigilant understanding of the spectrum of macrofollicular thyroid disease for accurate diagnosis. ETV6::NTRK3 or other fusions, when found, present opportunities for targeted therapy.
Keywords: Cytology; IEFVPTC; Macrofollicular invasive encapsulated follicular variant of papillary thyroid carcinoma; Molecular; Radiology; Thyroid cancer.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Macrofollicular Variant of Follicular Thyroid Carcinoma: A Rare Underappreciated Pitfall in the Diagnosis of Thyroid Carcinoma.Thyroid. 2020 Jan;30(1):72-80. doi: 10.1089/thy.2018.0607. Epub 2019 Dec 30. Thyroid. 2020. PMID: 31701808
-
Macrofollicular variant of papillary carcinoma: a potential thyroid FNA pitfall.Diagn Cytopathol. 2007 Sep;35(9):560-4. doi: 10.1002/dc.20702. Diagn Cytopathol. 2007. PMID: 17703452
-
Fine-needle aspiration of the macrofollicular and microfollicular subtypes of the follicular variant of papillary carcinoma of the thyroid.Cancer. 1998 Aug 25;84(4):235-44. Cancer. 1998. PMID: 9723599
-
Macrofollicular variant of papillary thyroid carcinoma with extensive lymph node metastases.Endocr Pathol. 2014 Sep;25(3):265-72. doi: 10.1007/s12022-014-9306-y. Endocr Pathol. 2014. PMID: 24671758 Review.
-
Macrofollicular variant of papillary carcinoma of the thyroid: a histologic, cytologic, and immunohistochemical study of 3 cases and review of the literature.Arch Pathol Lab Med. 2004 Jan;128(1):54-8. doi: 10.5858/2004-128-54-MVOPCO. Arch Pathol Lab Med. 2004. PMID: 14692811 Review.
Cited by
-
Prognosis of invasive encapsulated follicular variant and classical papillary thyroid carcinoma: a propensity score-matched study using the SEER database.Sci Rep. 2025 Jan 2;15(1):413. doi: 10.1038/s41598-024-84425-w. Sci Rep. 2025. PMID: 39747560 Free PMC article.
-
The diagnostic and therapeutic process of invasive encapsulated follicular variant of papillary thyroid carcinoma with lung metastasis: a case report.Am J Transl Res. 2025 May 15;17(5):3560-3564. doi: 10.62347/LROE2153. eCollection 2025. Am J Transl Res. 2025. PMID: 40535669 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
