

Real-world data emulating randomized controlled trials of non-vitamin K antagonist oral anticoagulants in patients with venous thromboembolism
- PMID: 37775786
- PMCID: PMC10542685
- DOI: 10.1186/s12916-023-03069-1
Real-world data emulating randomized controlled trials of non-vitamin K antagonist oral anticoagulants in patients with venous thromboembolism
Abstract
Background: Emulating randomized controlled trials (RCTs) by real-world evidence (RWE) studies would benefit future clinical and regulatory decision-making by balancing the limitations of RCT. We aimed to evaluate whether the findings from RWE studies can support regulatory decisions derived from RCTs of non-vitamin K antagonist oral anticoagulants (NOACs) in patients with venous thromboembolism (VTE).
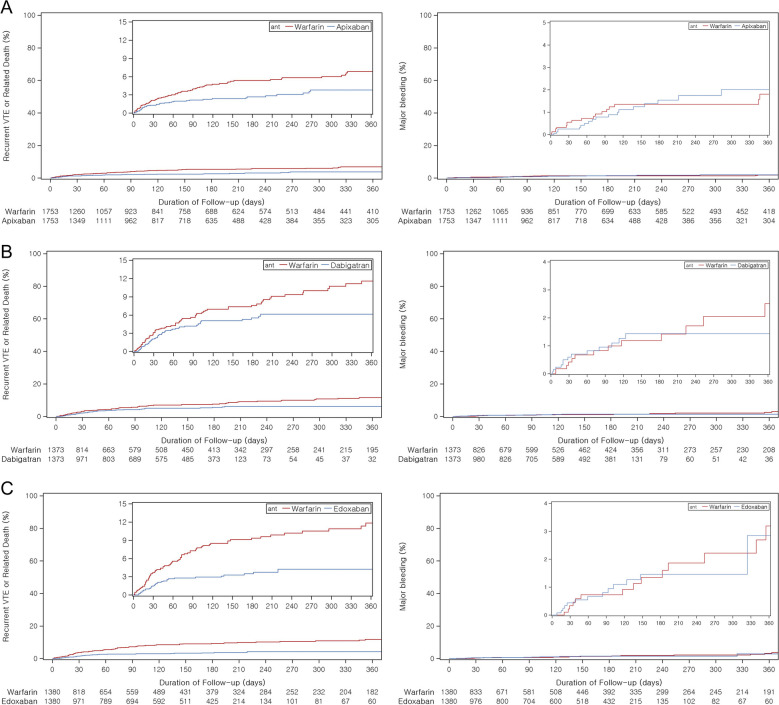
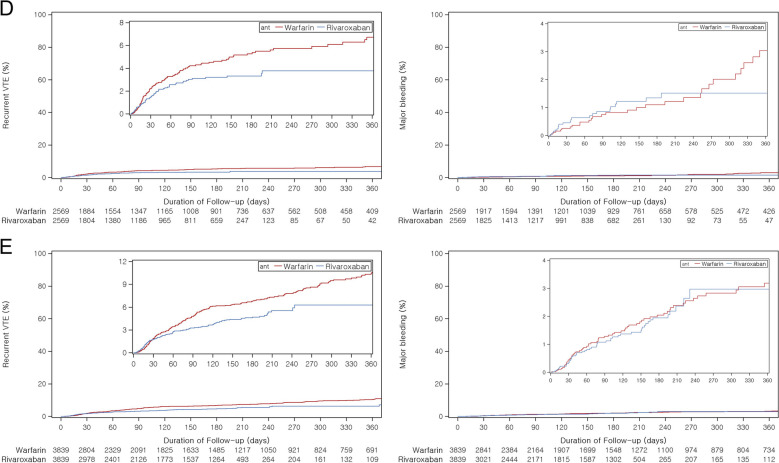
Methods: Five landmark trials (AMPLIFY, RE-COVER II, Hokusai-VTE, EINSTEIN-DVT, and EINSTEIN-PE) of NOACs were emulated using the South Korean nationwide claims database (January 2012 to August 2020). We applied an active comparator and new-user design to include patients who initiated oral anticoagulants within 28 days from their VTE diagnoses. The prespecified eligibility criteria, exposure (each NOAC, such as apixaban, rivaroxaban, dabigatran, and edoxaban), comparator (conventional therapy, defined as subcutaneous heparin followed by warfarin), and the definition of outcomes from RCTs were emulated as closely as possible in each separate emulation cohort. The primary outcome was identical to each trial, which was defined as recurrent VTE or VTE-related death. The safety outcome was major bleeding. Propensity score matching was conducted to balance 69 covariates between the exposure groups. Effect estimates for outcomes were estimated using the Mantel-Haenszel method and Cox proportional hazards model and subsequently compared with the corresponding RCT estimates.
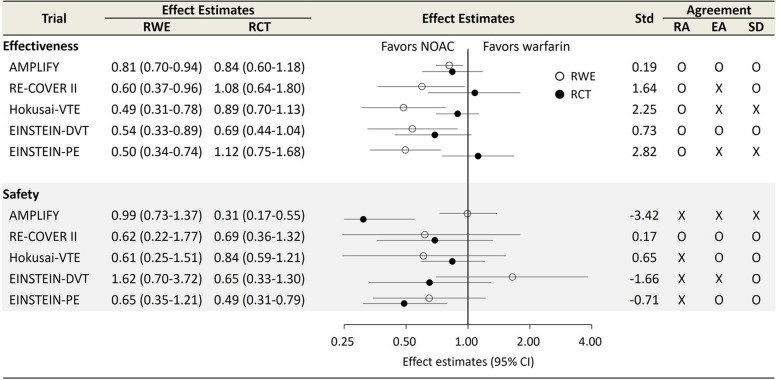
Results: Compared to trial populations, real-world study populations were older (range: 63-69 years [RWE] vs. 54-59 years [RCT]), with more females (55-60.5% vs. 39-48.3%) and had a higher prevalence of active cancer (4.2-15.4% vs. 2.5-9.5%). The emulated estimates for effectiveness outcomes showed superior effectiveness of NOAC (AMPLIFY: relative risk 0.81, 95% confidence interval 0.70-0.94; RE-COVER II: hazard ratio [HR] 0.60, 0.37-0.96; Hokusai-VTE: 0.49, 0.31-0.78; EINSTEIN-DVT: 0.54, 0.33-0.89; EINSTEIN-PE: 0.50, 0.34-0.74), when contrasted with trials that showed non-inferiority. For safety outcomes, all emulations except for AMPLIFY and EINSTEIN-DVT yielded results consistent with their corresponding RCTs.
Conclusions: This study revealed the feasibility of complementing RCTs with RWE studies by using claims data in patients with VTE. Future studies to consider the different demographic characteristics between RCT and RWE populations are needed.
Keywords: Anticoagulants; Clinical trials; Epidemiologic methods; Factor Xa inhibitors; Venous thromboembolism.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form. All authors have financial support from the Government-wide R&D Fund Project for Infectious Disease Research (Grant no. HG18C0068). Dr. Shin received grants from the Ministry of Food and Drug Safety, the Ministry of Health and Welfare, the National Research Foundation of Korea, and the Government-wide R&D Fund for Infectious Disease Research and Pharmaceutical Companies, including Amgen, Pfizer, SK Bioscience, Daiichi Sankyo, and GSK. No other relationships or activities have influenced the submitted work. Dr. Park is supported by the AIR@innoHK program of the Government of Hong Kong Special Administrative Region Innovation and Technology Commission. Others declare that they have no competing interests.
Figures
References
-
- Franklin JM, Patorno E, Desai RJ, Glynn RJ, Martin D, Quinto K, Pawar A, Bessette LG, Lee H, Garry EM, et al. Emulating randomized clinical trials with nonrandomized real-world evidence studies: first results from the RCT DUPLICATE Initiative. Circulation. 2021;143(10):1002–1013. doi: 10.1161/CIRCULATIONAHA.120.051718. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
