

Severe Fontan-Associated Liver Disease and Its Association With Mortality
- PMID: 37776221
- PMCID: PMC10727255
- DOI: 10.1161/JAHA.121.024034
Severe Fontan-Associated Liver Disease and Its Association With Mortality
Abstract
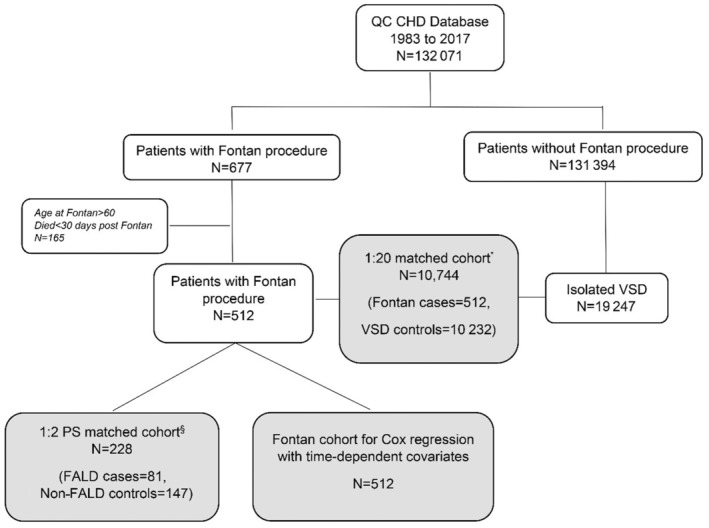
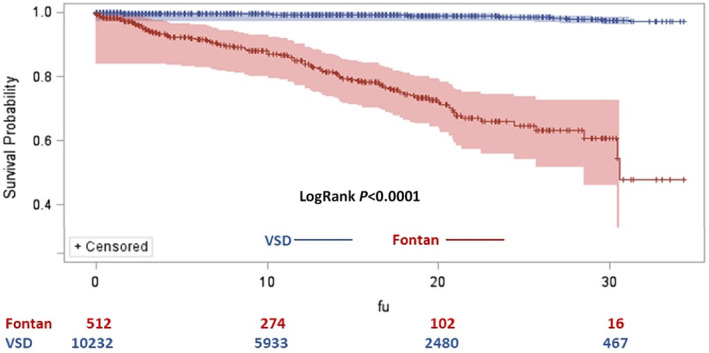
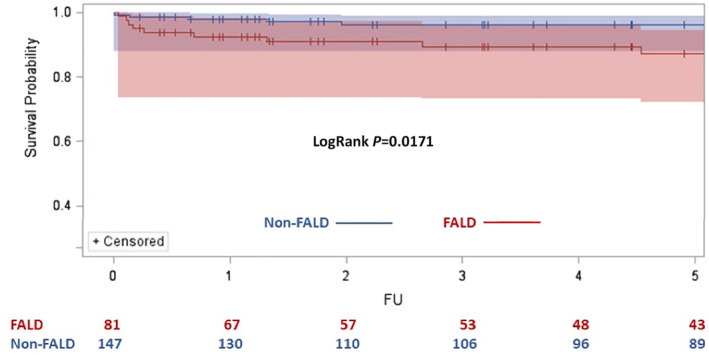
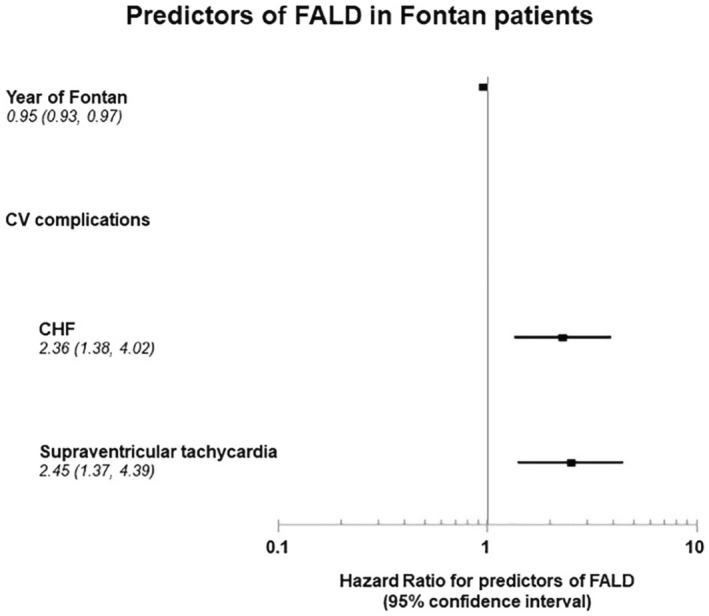
Background Data are rare about the incidence of severe Fontan-associated liver disease (FALD) and its association with mortality. We sought to: (1) estimate the probability of developing severe FALD in patients who undergo the Fontan procedure (Fontan patients), compared with severe liver complications in patients with a ventricular septal defect; (2) assess the severe FALD-mortality association; and (3) identify risk factors for developing severe FALD. Methods and Results Using the Quebec Congenital Heart Disease database, a total of 512 Fontan patients and 10 232 patients with a ventricular septal defect were identified. Kaplan-Meier curves demonstrated significantly higher cumulative risk of severe FALD in Fontan patients (11.95% and 52.24% at 10 and 35 years, respectively), than the risk of severe liver complications in patients with a ventricular septal defect (0.50% and 2.75%, respectively). At 5 years, the cumulative risk of death was 12.60% in patients with severe FALD versus 3.70% in Fontan patients without FALD (log-rank P=0.0171). Cox proportional hazard models identified significant associations between the development of severe FALD and congestive heart failure and supraventricular tachycardia, with hazard ratios (HRs) of 2.36 (95% CI, 1.38-4.02) and 2.45 (95% CI, 1.37-4.39), respectively. More recent Fontan completion was related to reduced risks of severe FALD, with an HR of 0.95 (95% CI, 0.93-0.97) for each more recent year. Conclusions This large-scale population-based study documents that severe FALD in Fontan patients was associated with a >3-fold increase in mortality. The risk of FALD is time-dependent and can reach >50% by 35 years after the Fontan operation. Conditions promoting poor Fontan hemodynamics were associated with severe FALD development.
Keywords: Fontan procedure; congenital heart defects; liver diseases; mortality; risk factor.
Figures
Comment in
-
Fontan Associated Liver Disease: Canary in the Coal Mine or Silent Killer?J Am Heart Assoc. 2023 Oct 3;12(19):e031597. doi: 10.1161/JAHA.123.031597. Epub 2023 Sep 30. J Am Heart Assoc. 2023. PMID: 37776191 Free PMC article. No abstract available.
References
-
- Daniels CJ, Bradley EA, Landzberg MJ, Aboulhosn J, Beekman RH, Book W, Gurvitz M, John A, John B, Marelli A, et al. Fontan‐associated liver disease: proceedings from the American College of Cardiology Stakeholders Meeting, October 1 to 2, 2015, Washington DC. J Am Coll Cardiol. 2017;70:3173–3194. doi: 10.1016/j.jacc.2017.10.045 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
