

Complex Percutaneous Coronary Intervention Outcomes in Older Adults
- PMID: 37776222
- PMCID: PMC10727245
- DOI: 10.1161/JAHA.122.029057
Complex Percutaneous Coronary Intervention Outcomes in Older Adults
Abstract
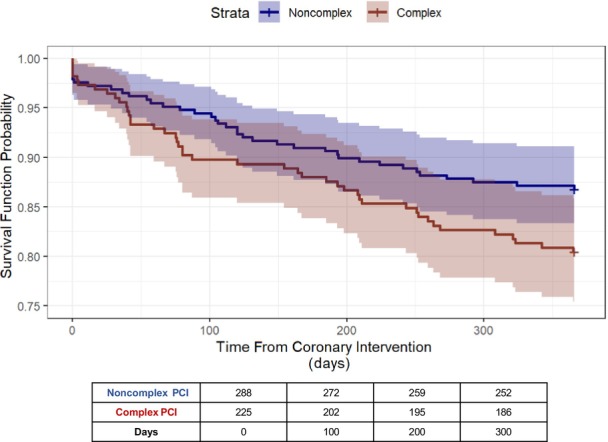
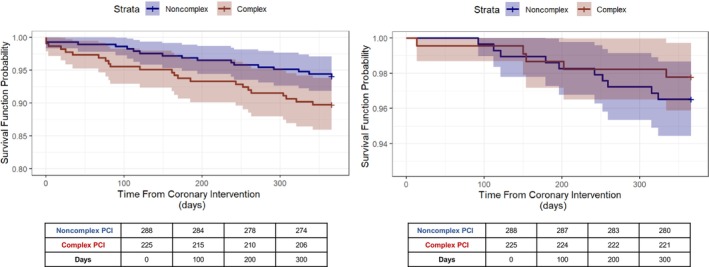
Background Complex percutaneous coronary intervention (PCI) is increasingly performed in older adults (age ≥75 years) with stable ischemic heart disease. However, little is known about clinical outcomes. Methods and Results We derived a cohort of older adults undergoing elective PCI for stable ischemic heart disease across a large health system. We compared 12-month event-free survival (freedom from all-cause death, nonfatal myocardial infarction, stroke, and major bleeding), all-cause death, target lesion revascularization, and bleeding events for patients receiving complex versus noncomplex PCI and derived risk estimates with Cox regression models. We included 513 patients (mean age, 81±5 years). Patients receiving complex PCI versus noncomplex PCI did not significantly differ across a host of clinical characteristics including cardiovascular disease features, noncardiac comorbidities, guideline-directed medical therapy use, and frailty. Patients receiving complex PCI versus noncomplex PCI experienced worse event-free survival (80.4% versus 86.8%), which was not significant in adjusted analyses (hazard ratio [HR], 1.38 [95% CI, 0.88-2.16]). All-cause death at 1 year for patients undergoing complex PCI was nearly double that seen for patients receiving noncomplex PCI (10.2% versus 5.9%), and the risk was significant in models adjusted for clinical characteristics (HR, 1.97 [95% CI, 1.02-3.79]). Target lesion revascularization risk was lower for patients receiving complex PCI (2.2% versus 3.5%, adjusted HR), but bleeding events were not statistically different between groups (25.3% versus 20.5%; P=0.19). Conclusions Complex PCI in older adults with stable ischemic heart disease was associated with lower risk of target lesion revascularization but higher all-cause death compared with noncomplex PCI.
Keywords: complex percutaneous coronary intervention; coronary artery disease; older adults; revascularization.
Figures
Comment in
-
Another Piece of the Complex Puzzle: Outcomes of Percutaneous Coronary Intervention in Older Adults.J Am Heart Assoc. 2023 Oct 3;12(19):e031827. doi: 10.1161/JAHA.123.031827. Epub 2023 Sep 30. J Am Heart Assoc. 2023. PMID: 37776215 Free PMC article. No abstract available.
References
-
- Heron M. Deaths: leading causes for 2019. Natl Vital Stat Rep. 2021;70:1–114. - PubMed
-
- Tegn N, Abdelnoor M, Aaberge L, Endresen K, Smith P, Aakhus S, Gjertsen E, Dahl‐Hofseth O, Ranhoff AH, Gullestad L, et al. Invasive versus conservative strategy in patients aged 80 years or older with non‐ST‐elevation myocardial infarction or unstable angina pectoris (After Eighty study): an open‐label randomised controlled trial. Lancet. 2016;387:1057–1065. doi: 10.1016/S0140-6736(15)01166-6 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
