

Elevated remnant cholesterol and atherosclerotic cardiovascular disease in diabetes: a population-based prospective cohort study
- PMID: 37776347
- PMCID: PMC10627991
- DOI: 10.1007/s00125-023-06016-0
Elevated remnant cholesterol and atherosclerotic cardiovascular disease in diabetes: a population-based prospective cohort study
Abstract
Aims/hypothesis: Elevated remnant cholesterol is observationally and causally associated with increased risk of atherosclerotic cardiovascular disease (ASCVD) in the general population. This association is not well studied in individuals with diabetes, who are often included in clinical trials of remnant cholesterol-lowering therapy. We tested the hypothesis that elevated remnant cholesterol is associated with increased risk of ASCVD in individuals with diabetes. We also explored the fraction of excess risk conferred by diabetes which can be explained by elevated remnant cholesterol.
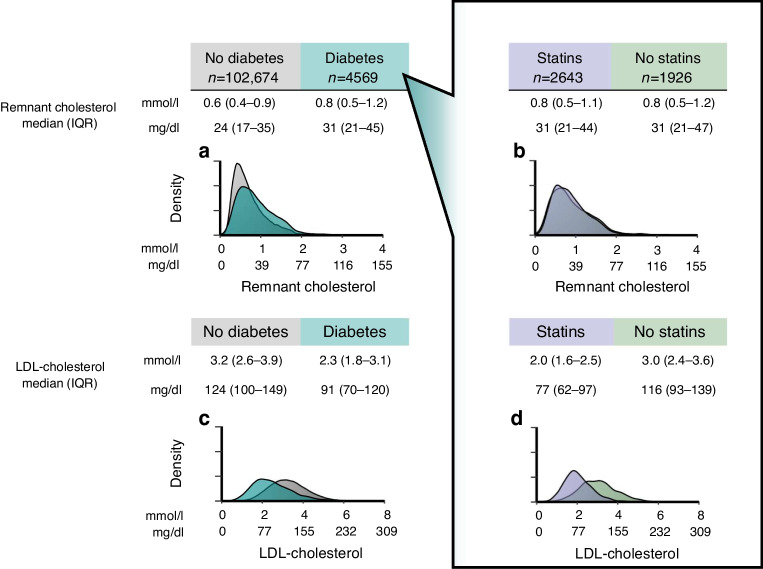
Methods: We included 4569 white Danish individuals with diabetes (58% statin users) nested within the Copenhagen General Population Study (2003-2015). The ASCVDs peripheral artery disease, myocardial infarction and ischaemic stroke were extracted from national Danish health registries without losses to follow-up. Remnant cholesterol was calculated from a standard lipid profile.
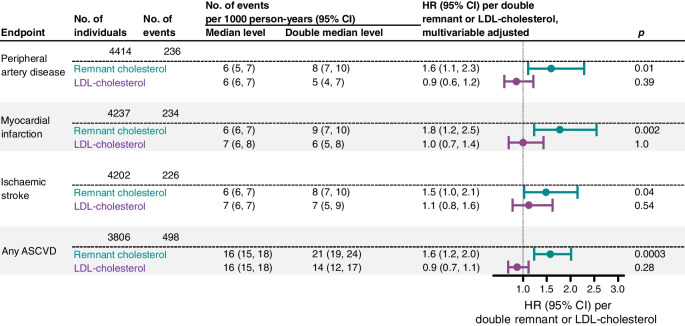
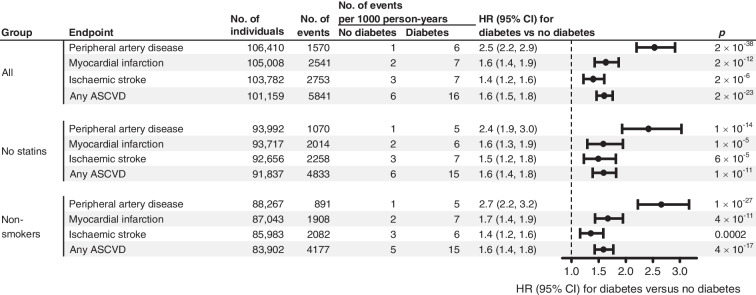
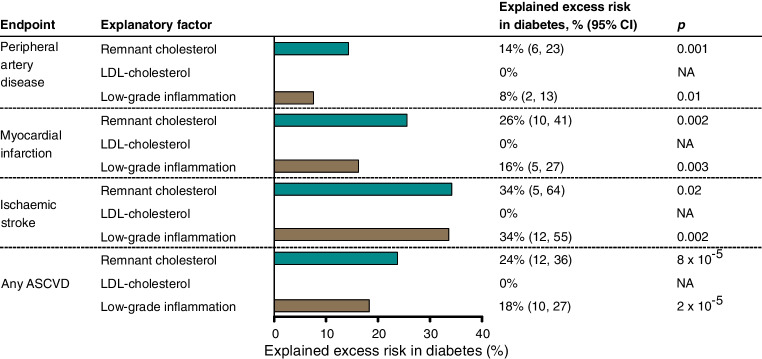
Results: During up to 15 years of follow-up, 236 individuals were diagnosed with peripheral artery disease, 234 with myocardial infarction, 226 with ischaemic stroke and 498 with any ASCVD. Multivariable adjusted HR (95% CI) per doubling of remnant cholesterol was 1.6 (1.1, 2.3; p=0.01) for peripheral artery disease, 1.8 (1.2, 2.5; p=0.002) for myocardial infarction, 1.5 (1.0, 2.1; p=0.04) for ischaemic stroke, and 1.6 (1.2, 2.0; p=0.0003) for any ASCVD. Excess risk conferred by diabetes was 2.5-fold for peripheral artery disease, 1.6-fold for myocardial infarction, 1.4-fold for ischaemic stroke and 1.6-fold for any ASCVD. Excess risk explained by elevated remnant cholesterol and low-grade inflammation was 14% and 8% for peripheral artery disease, 26% and 16% for myocardial infarction, 34% and 34% for ischaemic stroke, and 24% and 18% for any ASCVD, respectively. LDL-cholesterol did not explain excess risk, as it was not higher in individuals with diabetes. We also explored the fraction of excess risk conferred by diabetes which can be explained by elevated remnant cholesterol.
Conclusions/interpretation: Elevated remnant cholesterol was associated with increased risk of ASCVD in individuals with diabetes. Remnant cholesterol and low-grade inflammation explained substantial excess risk of ASCVD conferred by diabetes. Whether remnant cholesterol should be used as a treatment target remains to be determined in randomised controlled trials.
Keywords: Impaired glucose tolerance; Insulin resistance; Lower-extremity arterial disease; Triglyceride-rich lipoprotein; Very-low-density lipoprotein.
© 2023. The Author(s).
Conflict of interest statement
BGN reports consultancies and talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Ionis, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Esperion, Abbott and Silence Therapeutics. There are no competing interests for BNW, KMP or ABW.
Figures
References
-
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157:107843. doi: 10.1016/j.diabres.2019.107843. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
