

Multi-omics analysis of mucosal and systemic immunity to SARS-CoV-2 after birth
- PMID: 37776858
- PMCID: PMC10724861
- DOI: 10.1016/j.cell.2023.08.044
Multi-omics analysis of mucosal and systemic immunity to SARS-CoV-2 after birth
Abstract
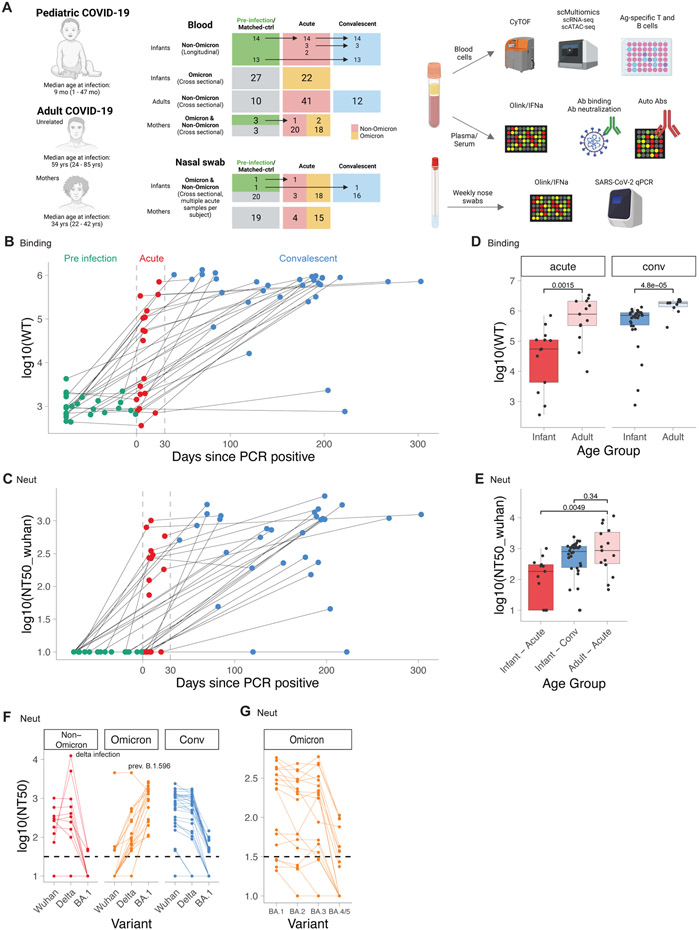
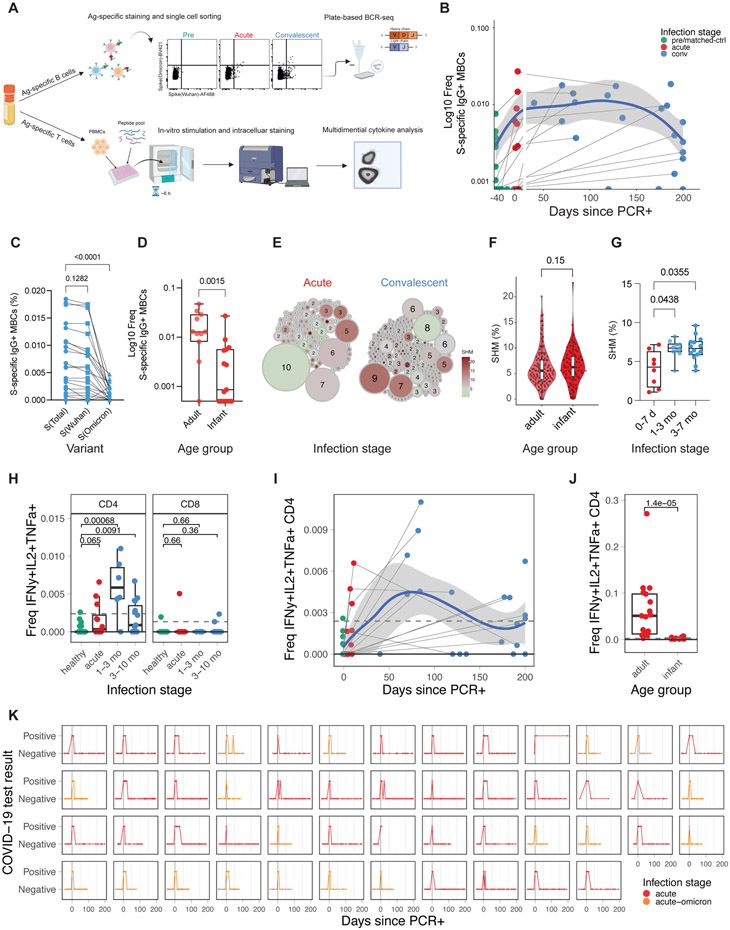
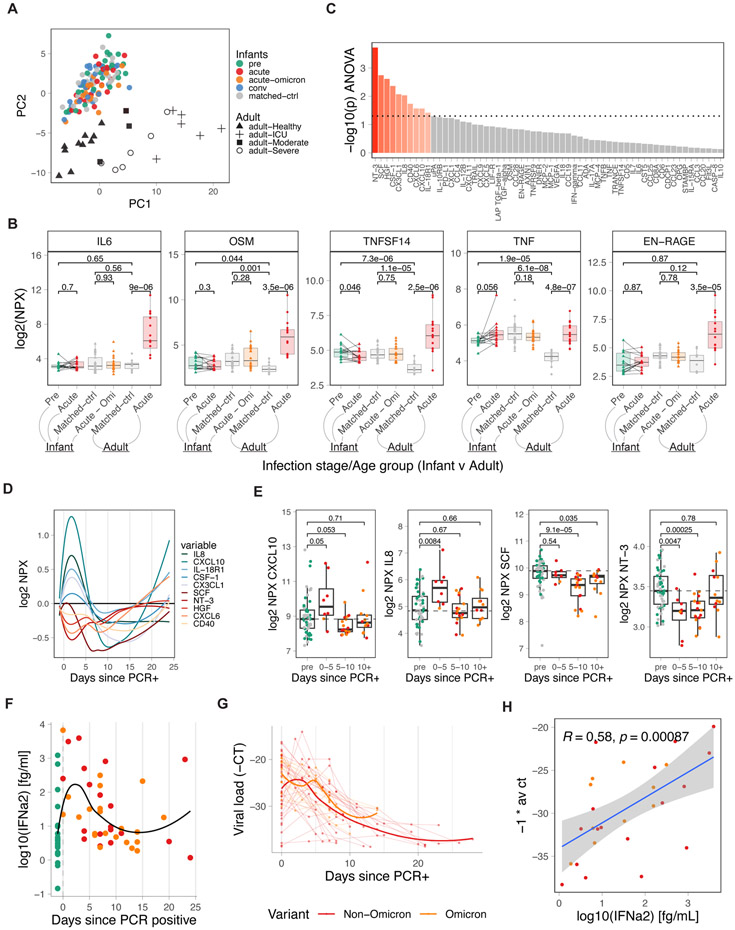
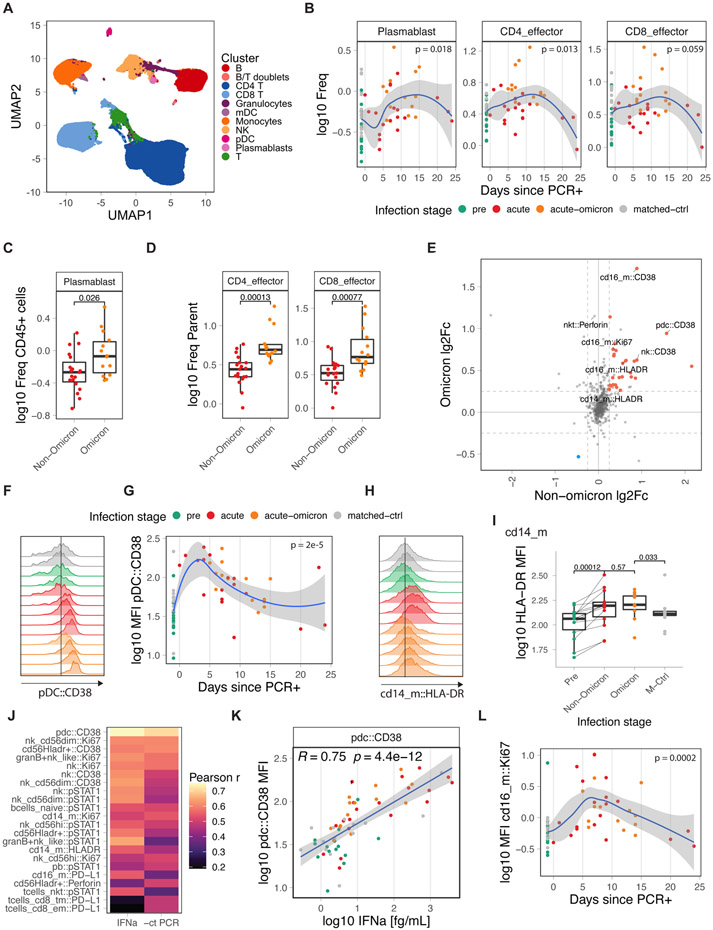
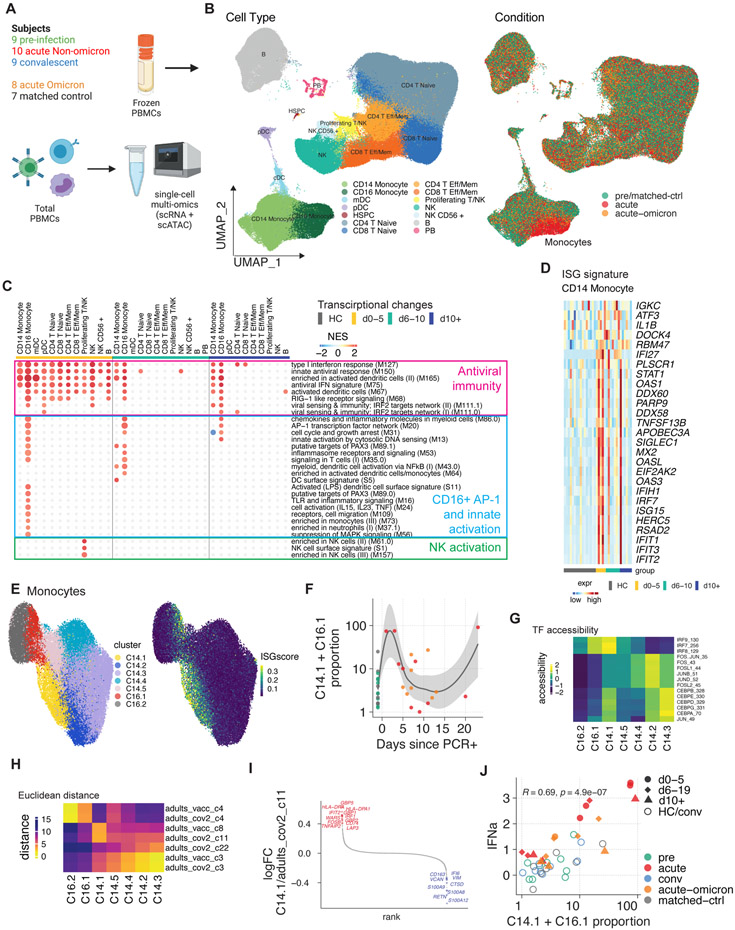
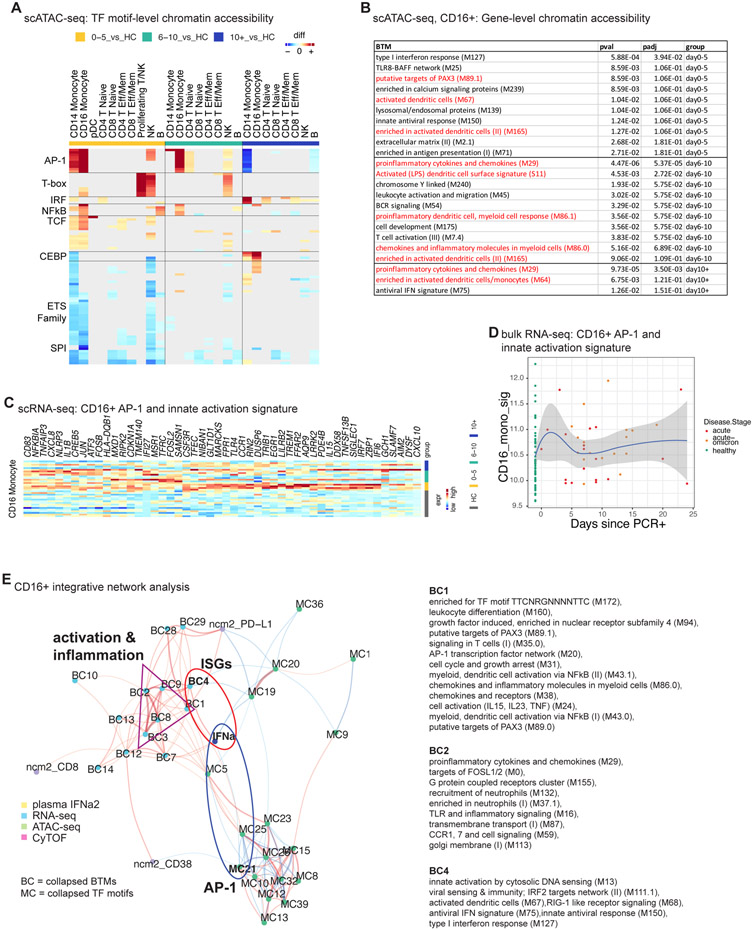
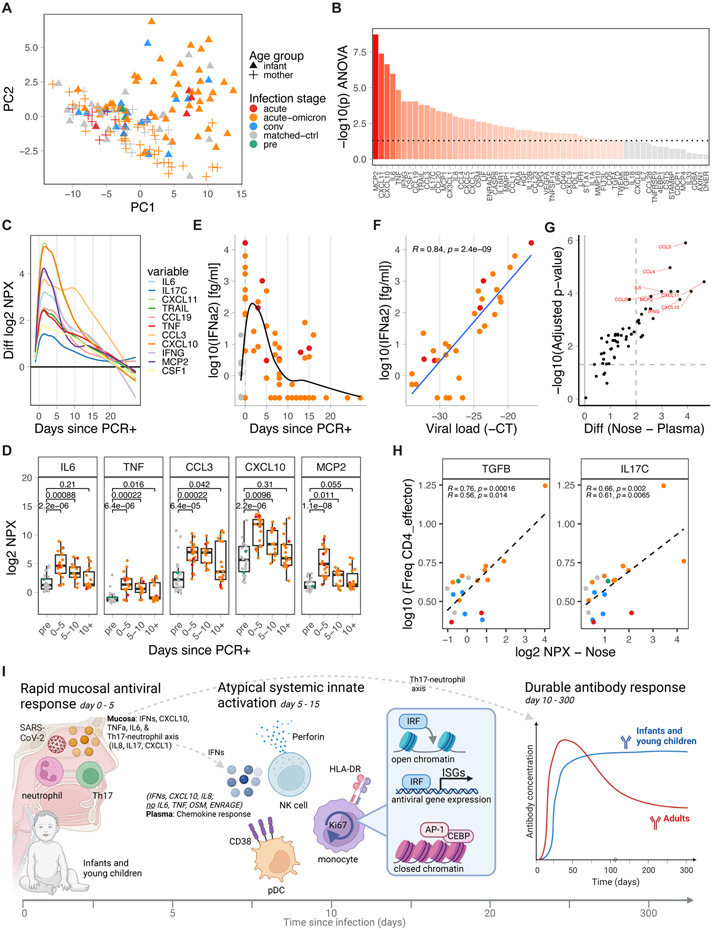
The dynamics of immunity to infection in infants remain obscure. Here, we used a multi-omics approach to perform a longitudinal analysis of immunity to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in infants and young children by analyzing blood samples and weekly nasal swabs collected before, during, and after infection with Omicron and non-Omicron variants. Infection stimulated robust antibody titers that, unlike in adults, showed no sign of decay for up to 300 days. Infants mounted a robust mucosal immune response characterized by inflammatory cytokines, interferon (IFN) α, and T helper (Th) 17 and neutrophil markers (interleukin [IL]-17, IL-8, and CXCL1). The immune response in blood was characterized by upregulation of activation markers on innate cells, no inflammatory cytokines, but several chemokines and IFNα. The latter correlated with viral load and expression of interferon-stimulated genes (ISGs) in myeloid cells measured by single-cell multi-omics. Together, these data provide a snapshot of immunity to infection during the initial weeks and months of life.
Keywords: SARS-CoV-2; durability; infants; mucosal immunity; multi-omics; neonates; single-cell ATAC-seq; single-cell RNA-seq; viral infection.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests B.P. serves on the External Immunology Board of GSK and on the Scientific Advisory Board of Sanofi, Medicago, Boehringer Ingelheim, Icosavax, and EdJen. F.W. is a consultant for Gilead. A.S. is a consultant for Gritstone Bio, Flow Pharma, Moderna, AstraZeneca, Qiagen, Fortress, Gilead, Sanofi, Merck, RiverVest, MedaCorp, Turnstone, NA Vaccine Institute, Emervax, Gerson Lehrman Group and Guggenheim. LJI has filed for patent protection for various aspects of T cell epitope and vaccine design work.
Figures
References
-
- Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, Rovida F, Baldanti F, and Marseglia GL (2020). Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr. 174, 882–889. 10.1001/jamapediatrics.2020.1467. - DOI - PubMed
-
- Provisional COVID-19 Deaths: Focus on Ages 0–18 Years ∣ Data ∣ Centers for Disease Control and Prevention. https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-Focus-on-Ages-0-18....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
