

A combined clinical and specific genes' model to predict live birth for in vitro fertilization and embryo transfer patients
- PMID: 37777726
- PMCID: PMC10541716
- DOI: 10.1186/s12884-023-05988-6
A combined clinical and specific genes' model to predict live birth for in vitro fertilization and embryo transfer patients
Abstract
Background: We aimed to develop an accurate model to predict live birth for patients receiving in vitro fertilization and embryo transfer (IVF-ET) treatment.
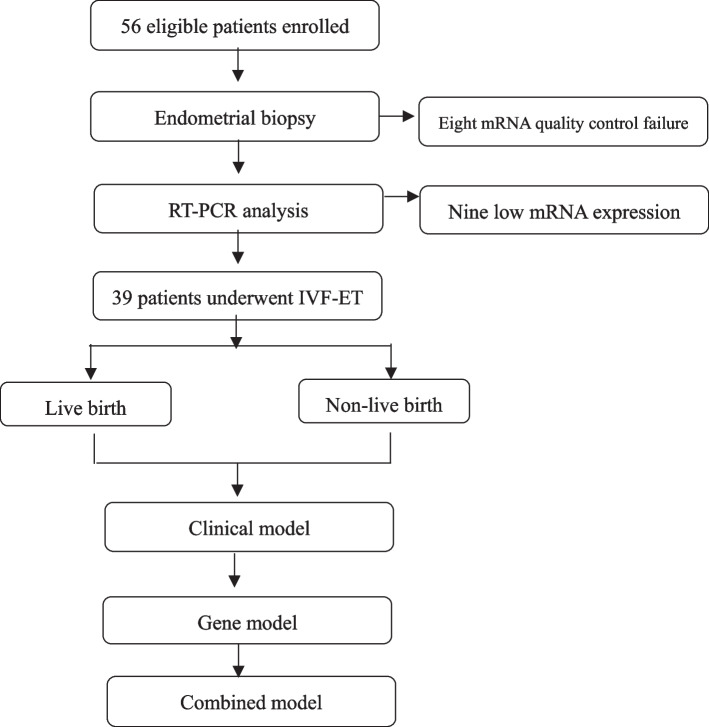
Methods: This is a prospective nested case-control study. Women aged between 18 and 38 years, whose body mass index (BMI) were between the range of 18.5-24 kg/m2, who had an endometrium of ≥ 8 mm at the thickest were enrolled from 2018/9 to 2020/8. All patients received IVF-ET treatment and were followed up until Jan. 2022 when they had reproductive outcomes. Endometrial samples during the window of implantation (LH + 6 to 9 days) were subjected to analyze specific endometrial receptivity genes' expression using real-time PCR (RT-PCR). Patients were divided into live birth group and non-live birth group based on IVF-ET outcomes. Clinical signatures relevant to live birth were collected, analyzed, and used to establish a predictive model for live birth by univariate analysis (clinical model). Specific endometrial receptivity genes' expression was analyzed, selected, and used to construct a predictive model for live birth by The Least Absolute Shrinkage and Selection Operator (LASSO) analysis (gene model). Finally, significant clinical factors and genes were used to construct a combined model for predicting live birth using multivariate logistical regression (combined model). Different models' Area Under Curve (AUC) were compared to identify the most predictive model.
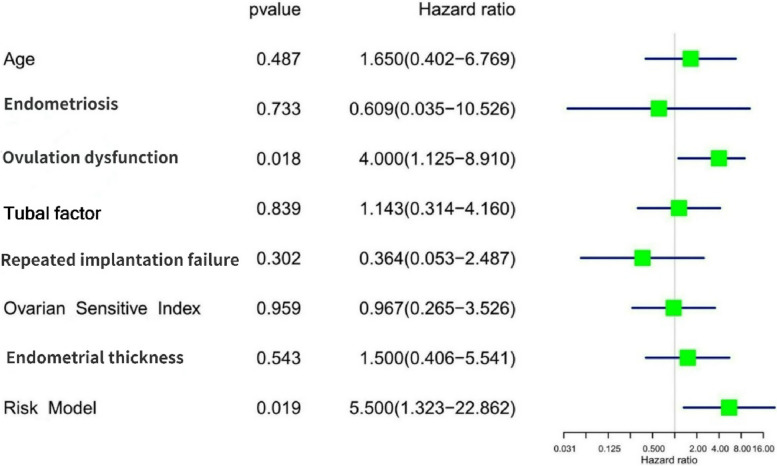
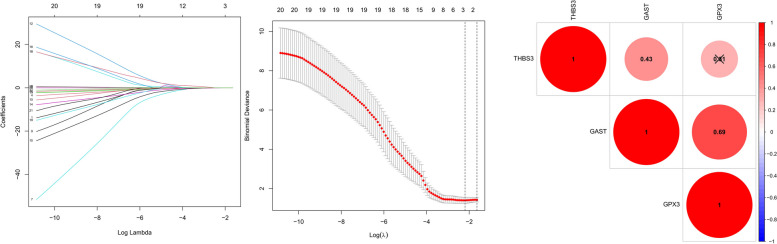
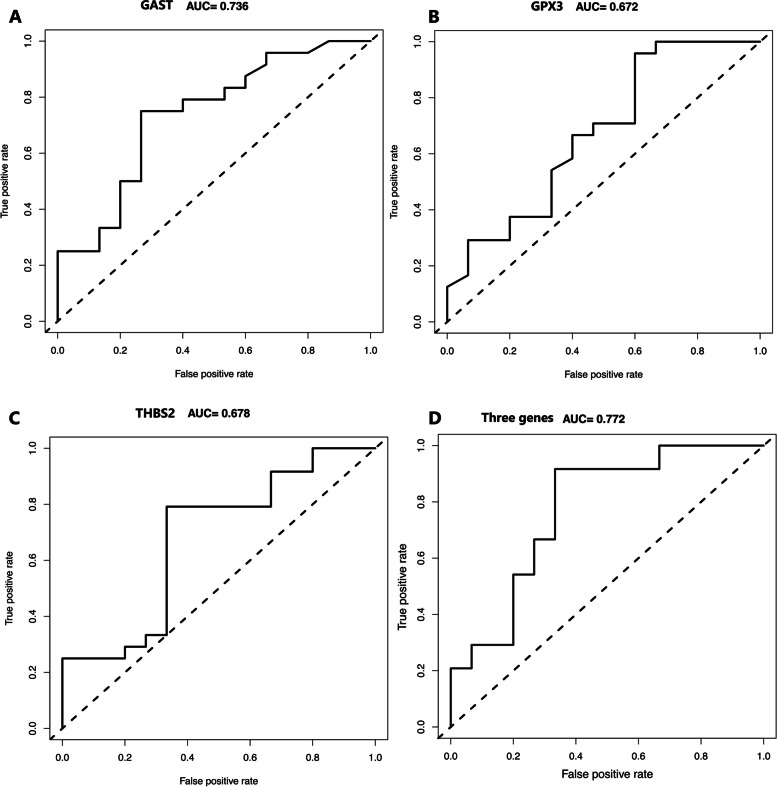
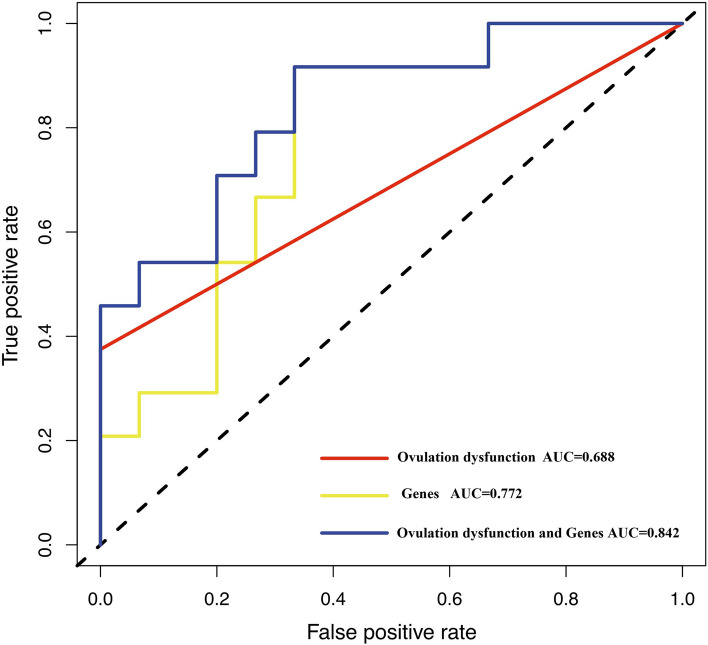
Results: Thirty-nine patients were enrolled in the study, twenty-four patients had live births, fifteen did not. In univariate analysis, the odds of live birth for women with ovulation dysfunction was 4 times higher than that for women with other IVF-ET indications (OR = 4.0, 95% CI: 1.125 - 8.910, P = 0.018). Age, body mass index, duration of infertility, primary infertility, repeated implantation failure, antral follicle counting, ovarian sensitivity index, anti-Mullerian hormone, controlled ovarian hyperstimulation protocol and duration, total dose of FSH/hMG, number of oocytes retrieved, regiment of endometrial preparation, endometrium thickness before embryo transfer, type of embryo transferred were not associated with live birth (P > 0.05). Only ovulation dysfunction was used to construct the clinical model and its AUC was 0.688. In lasso analysis, GAST, GPX3, THBS2 were found to promote the risk of live birth. AUCs for GAST, GPX3, THBS2 reached to 0.736, 0.672, and 0.678, respectively. The gene model was established based on these three genes and its AUC was 0.772. Ovulation dysfunction, GAST, GPX3, and THBS2 were finally used to construct the combined model, reaching the highest AUC (AUC = 0.842).
Conclusions: Compared to the single model, the combined model of clinical (Ovulation dysfunction) and specific genes (GAST, GPX3, THBS2) was more accurate to predict live birth for IVF-ET patients.
Keywords: Endometrial receptivity; Gene expression; LASSO regression; Live birth; Ovulation dysfunction.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
[Effect of domestic highly purified urinary follicle stimulating hormone on outcomes of in vitro fertilization-embryo transfer in controlled ovarian stimulation].Zhonghua Fu Chan Ke Za Zhi. 2013 Nov;48(11):838-42. Zhonghua Fu Chan Ke Za Zhi. 2013. PMID: 24444561 Chinese.
-
Salpingectomy may decrease antral follicle count but not live birth rate for IVF-ET patients aged 35-39 years: a retrospective study.J Ovarian Res. 2020 Jul 20;13(1):80. doi: 10.1186/s13048-020-00678-9. J Ovarian Res. 2020. PMID: 32684158 Free PMC article.
-
Relationship Between Anti-Müllerian Hormone and In Vitro Fertilization-Embryo Transfer in Clinical Pregnancy.Front Endocrinol (Lausanne). 2020 Dec 4;11:595448. doi: 10.3389/fendo.2020.595448. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33343511 Free PMC article.
-
Higher probability of live-birth in high, but not normal, responders after first frozen-embryo transfer in a freeze-only cycle strategy compared to fresh-embryo transfer: a meta-analysis.Hum Reprod. 2019 Mar 1;34(3):491-505. doi: 10.1093/humrep/dey388. Hum Reprod. 2019. PMID: 30689865
-
Endometrial injury in women undergoing in vitro fertilisation (IVF).Cochrane Database Syst Rev. 2021 Jun 10;6(6):CD009517. doi: 10.1002/14651858.CD009517.pub4. Cochrane Database Syst Rev. 2021. PMID: 34110001 Free PMC article.
Cited by
-
Seasonal environmental fluctuations alter the transcriptome dynamics of oocytes and granulosa cells in beef cows.J Ovarian Res. 2024 Oct 14;17(1):201. doi: 10.1186/s13048-024-01530-0. J Ovarian Res. 2024. PMID: 39402580 Free PMC article.
References
-
- Vaegter KK, Lakic TG, Olovsson M, Berglund L, Brodin T, Holte J. Which factors are most predictive for live birth after in vitro fertilization and intracytoplasmic sperm injection (IVF/ICSI) treatments? Analysis of 100 prospectively recorded variables in 8,400 IVF/ICSI single-embryo transfers. Fertil Steril. 2017;107(3):641–648.e2. doi: 10.1016/j.fertnstert.2016.12.005. - DOI - PubMed
-
- Díaz-Gimeno P, Ruiz-Alonso M, Blesa D, Bosch N, Martínez-Conejero JA, Alama P, et al. The accuracy and reproducibility of the endometrial receptivity array is superior to histological dating as diagnostic method for the endometrial factor. Fertil Steril. 2013;99:508–517. doi: 10.1016/j.fertnstert.2012.09.046. - DOI - PubMed
-
- Alonso MR, et al. Clinical efficiency of embryo transfer performed in receptive vs non-receptive endometrium diagnosed by the endometrial receptivity array (era) test. Fertil Steril. 2014;102(3):e292. doi: 10.1016/j.fertnstert.2014.07.994. - DOI
MeSH terms
Grants and funding
- 2019-Q-01/the cooperative supported project of the People's Hospital of Peking University and Zoology
- 2019-Q-01/the cooperative supported project of the People's Hospital of Peking University and Zoology
- 2019-Q-01/the cooperative supported project of the People's Hospital of Peking University and Zoology
- 2018-2-4085/Capital Health Development Scientific Research Project
- 2018-2-4085/Capital Health Development Scientific Research Project
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
