

A randomized phase II trial of MR-guided prostate stereotactic body radiotherapy administered in 5 or 2 fractions for localized prostate cancer (FORT)
- PMID: 37777738
- PMCID: PMC10544147
- DOI: 10.1186/s12885-023-11430-z
A randomized phase II trial of MR-guided prostate stereotactic body radiotherapy administered in 5 or 2 fractions for localized prostate cancer (FORT)
Abstract
Background: Ultra-hypofractionated regimens for definitive prostate cancer (PCa) radiotherapy are increasingly utilized due in part to promising safety and efficacy data complemented by greater patient convenience from a treatment course requiring fewer sessions. As such, stereotactic body radiation therapy (SBRT) is rapidly emerging as a standard definitive treatment option for patients with localized PCa. The commercially available magnetic resonance linear accelerator (MR-LINAC) integrates MR imaging with radiation delivery, providing several theoretical advantages compared to computed tomography (CT)-guided radiotherapy. MR-LINAC technology facilitates improved visualization of the prostate, real-time intrafraction tracking of prostate and organs-at-risk (OAR), and online adaptive planning to account for target movement and anatomical changes. These features enable reduced treatment volume margins and improved sparing of surrounding OAR. The theoretical advantages of MR-guided radiotherapy (MRgRT) have recently been shown to significantly reduce rates of acute grade ≥ 2 GU toxicities as reported in the prospective randomized phase III MIRAGE trial, which compared MR-LINAC vs CT-based 5 fraction SBRT in patients with localized PCa (Kishan et al. JAMA Oncol 9:365-373, 2023). Thus, MR-LINAC SBRT-utilizing potentially fewer treatments-is warranted and clinically relevant for men with low or intermediate risk PCa electing for radiotherapy as definitive treatment.
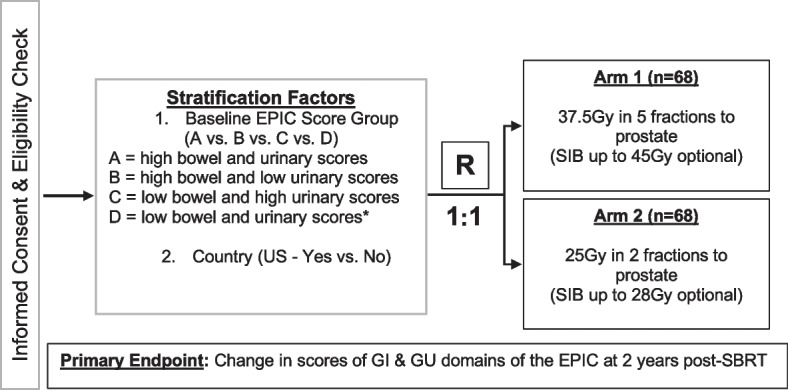
Methods/design: A total of 136 men with treatment naïve low or intermediate risk PCa will be randomized in a 1:1 ratio to 5 or 2 fractions of MR-guided SBRT using permuted block randomization. Randomization is stratified by baseline Expanded PCa Index Composite (EPIC) bowel and urinary domain scores. Patients undergoing 5 fractions will receive 37.5 Gy to the prostate over 10-14 days and patients undergoing 2 fractions will receive 25 Gy to the prostate over 7-10 days. The co-primary endpoints are GI and GU toxicities as measured by change scores in the bowel and urinary EPIC domains, respectively. The change scores will be calculated as pre-treatment (baseline) score subtracted from the 2-year score.
Discussion: FORT is an international, multi-institutional prospective randomized phase II trial evaluating whether MR-guided SBRT delivered in 2 fractions versus 5 fractions is non-inferior from a gastrointestinal (GI) and genitourinary (GU) toxicity standpoint at 2 years post-treatment in men with low or intermediate risk PCa.
Trial registration: Clinicaltrials.gov identifier: NCT04984343 . Date of registration: July 30, 2021.
Protocol version: 4.0, Nov 8, 2022.
Keywords: Definitive radiotherapy; Gastrointestinal (GI); Genitourinary (GU); MR-guided radiotherapy (MRgRT); Magnetic resonance linear accelerator (MR-LINAC); Prostate cancer (PCa); Stereotactic body radiotherapy (SBRT); Toxicity; Ultra-hypofractionation.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Randomized phase II trial of MRI-guided salvage radiotherapy for prostate cancer in 4 weeks versus 2 weeks (SHORTER).BMC Cancer. 2023 Aug 22;23(1):781. doi: 10.1186/s12885-023-11278-3. BMC Cancer. 2023. PMID: 37608258 Free PMC article. Clinical Trial.
-
Magnetic resonance imaging-guided stereotactic body radiotherapy for prostate cancer (mirage): a phase iii randomized trial.BMC Cancer. 2021 May 11;21(1):538. doi: 10.1186/s12885-021-08281-x. BMC Cancer. 2021. PMID: 33975579 Free PMC article. Clinical Trial.
-
Magnetic Resonance Imaging-Guided vs Computed Tomography-Guided Stereotactic Body Radiotherapy for Prostate Cancer: The MIRAGE Randomized Clinical Trial.JAMA Oncol. 2023 Mar 1;9(3):365-373. doi: 10.1001/jamaoncol.2022.6558. JAMA Oncol. 2023. PMID: 36633877 Free PMC article.
-
Acute toxicity comparison of magnetic resonance-guided adaptive versus fiducial or computed tomography-guided non-adaptive prostate stereotactic body radiotherapy: A systematic review and meta-analysis.Cancer. 2023 Oct 1;129(19):3044-3052. doi: 10.1002/cncr.34836. Epub 2023 Jul 24. Cancer. 2023. PMID: 37485697
-
MR-guided radiotherapy for prostate cancer: an inevitable transition?Curr Opin Urol. 2025 Sep 1;35(5):562-567. doi: 10.1097/MOU.0000000000001315. Epub 2025 Jul 4. Curr Opin Urol. 2025. PMID: 40620056 Review.
Cited by
-
Efficacy and safety of online adaptive magnetic resonance-guided fractionated stereotactic radiotherapy for brain metastases in non-small cell lung cancer (GASTO-1075): a single-arm, phase 2 trial.EClinicalMedicine. 2025 Apr 9;82:103189. doi: 10.1016/j.eclinm.2025.103189. eCollection 2025 Apr. EClinicalMedicine. 2025. PMID: 40247887 Free PMC article.
-
Stereotactic Body Radiotherapy (SBRT) to Localised Prostate Cancer in the Era of MRI-Guided Adaptive Radiotherapy: Doses Delivered in the HERMES Trial Comparing Two- and Five-Fraction Treatments.Cancers (Basel). 2024 May 30;16(11):2073. doi: 10.3390/cancers16112073. Cancers (Basel). 2024. PMID: 38893193 Free PMC article.
-
Implant geometry and detection rates of prostate fiducial markers after transrectal ultrasound-guided perineal implantation for image-guided 6D-tracking in robotic stereotactic body radiotherapy.Strahlenther Onkol. 2025 Aug;201(8):818-827. doi: 10.1007/s00066-024-02363-y. Epub 2025 Feb 6. Strahlenther Onkol. 2025. PMID: 39915304 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
