

Timing of SGLT2i initiation after acute myocardial infarction
- PMID: 37777743
- PMCID: PMC10544140
- DOI: 10.1186/s12933-023-02000-5
Timing of SGLT2i initiation after acute myocardial infarction
Abstract
Background: Pharmacological post-MI treatment is routinely initiated at intensive/cardiac care units. However, solid evidence for an early start of these therapies is only available for dual platelet therapy and statins, whereas data on beta blockers and RAAS inhibitors are heterogenous and mainly limited to STEMI and heart failure patients. Recently, the EMMY trial provided the first evidence on the beneficial effects of SGLT2 inhibitors (SGLT2i) when initiated early after PCI. In patients with type 2 diabetes mellitus, SGLT2i are considered "sick days drugs" and it, therefore, remains unclear if very early SGLT2i initiation following MI is as safe and effective as delayed initiation.
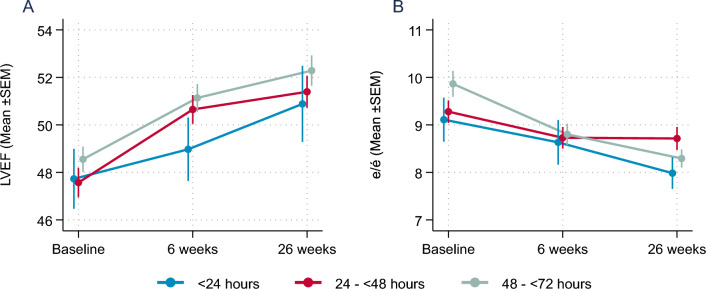
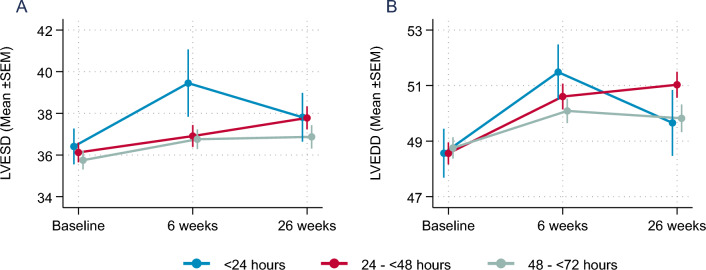
Methods and results: The EMMY trial evaluated the effect of empagliflozin on NT-proBNP and functional and structural measurements. Within the Empagliflozin group, 22 (9.5%) received early treatment (< 24 h after PCI), 98 (42.2%) within a 24 to < 48 h window (intermediate), and 111 (48.1%) between 48 and 72 h (late). NT-proBNP levels declined by 63.5% (95%CI: - 69.1; - 48.1) in the early group compared to 61.0% (- 76.0; - 41.4) in the intermediate and 61.9% (- 70.8; - 45.7) in the late group (n.s.) within the Empagliflozin group with no significant treatment groups-initiation time interaction (pint = 0.96). Secondary endpoints of left ventricular function (LV-EF, e/e`) as well as structure (LVESD and LVEDD) were also comparable between the groups. No significant difference in severe adverse event rate between the initiation time groups was detected.
Conclusion: Very early administration of SGLT2i after acute myocardial infarction does not show disadvantageous signals with respect to safety and appears to be as effective in reducing NT-proBNP as well as improving structural and functional LV markers as initiation after 2-3 days.
Trial registration: ClinicalTrials.gov NCT03087773.
Keywords: Clinical trial; Myocardial infarction; SGLT2i; Timing.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
H.S. is on the advisory board and speakers bureau of by Boehringer Ingelheim, NovoNordisk, Sanofi-Aventis, Amgen, AstraZeneca, Bayer, Eli Lilly, Kapsch, MSD, and Daiichi Sankyo. D.V.L. is on the advisory board and speakers’ bureau of Abiomed, AstraZeneca, Bayer, Daiichi Sankyo, Orion, Sanofi, and Servier and receives consulting fees from Recardio Inc, Bayer, TLL, Vaxxinity Inc. R.R.H. reports research support from AstraZeneca, Bayer and Merck Sharp & Dohme, and personal fees from Anji Pharmaceuticals, AstraZeneca, Novartis, and Novo Nordisk. M.W. receives speaker fees from Bayer, Novartis and consulting fees from Radcliff Cardiology. J.M.S.M. received speaker or consultant fees from Chiesi, Boehringer Ingelheim, Biosensors, P&F, Gruenenthal, Bayer, Medtronic, and Boston Scientific within the last 3 years. D.M. receives consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, and Vifor, further he receives payment for lectures from AstraZeneca, Bayer, Boehringer Ingelheim, Vifor, and BMS. The remaining authors have no relevant conflict of interest.
Figures
Similar articles
-
Effect of sodium-glucose co-transporter 2 inhibitors (SGLT2i) on N-terminal pro-B-type natriuretic peptide (NT-proBNP) level and structural changes following myocardial infarction: A systematic review and meta-analysis.Int J Cardiol. 2024 Sep 1;410:132239. doi: 10.1016/j.ijcard.2024.132239. Epub 2024 Jun 7. Int J Cardiol. 2024. PMID: 38852858
-
EMMY: The continued expansion of clinical applications of SGLT2 inhibitors.Glob Cardiol Sci Pract. 2023 Jan 30;2023(1):e202305. doi: 10.21542/gcsp.2023.5. eCollection 2023 Jan 30. Glob Cardiol Sci Pract. 2023. PMID: 36890845 Free PMC article.
-
Effects of canagliflozin on NT-proBNP stratified by left ventricular diastolic function in patients with type 2 diabetes and chronic heart failure: a sub analysis of the CANDLE trial.Cardiovasc Diabetol. 2021 Sep 14;20(1):186. doi: 10.1186/s12933-021-01380-w. Cardiovasc Diabetol. 2021. PMID: 34521417 Free PMC article. Clinical Trial.
-
Effects of empagliflozin in different phases of diabetes mellitus-related cardiomyopathy: a prospective observational study.BMC Cardiovasc Disord. 2021 Apr 29;21(1):217. doi: 10.1186/s12872-021-02024-3. BMC Cardiovasc Disord. 2021. PMID: 33926386 Free PMC article.
-
Efficacy and Safety of Early Initiation of Sodium-Glucose Co-transporter-2 Inhibitors Following Acute Myocardial Infarction: A Systematic Review and Meta-analysis.touchREV Endocrinol. 2025 May;21(1):14-23. doi: 10.17925/EE.2025.21.1.1. Epub 2025 Feb 7. touchREV Endocrinol. 2025. PMID: 40485654 Free PMC article.
Cited by
-
Acute effects of empagliflozin on open-loop baroreflex function and urine output in streptozotocin-induced type 1 diabetic rats.J Physiol Sci. 2024 Sep 28;74(1):48. doi: 10.1186/s12576-024-00938-z. J Physiol Sci. 2024. PMID: 39342112 Free PMC article.
-
Impact of baseline ECG characteristics on changes in cardiac biomarkers and echocardiographic metrices after acute myocardial infarction treated with Empagliflozin.Sci Rep. 2024 Jul 2;14(1):15083. doi: 10.1038/s41598-024-64175-5. Sci Rep. 2024. PMID: 38956086 Free PMC article. Clinical Trial.
-
Effect of sodium glucose cotransporter 2 inhibitors on all cause death and rehospitalization for heart failure in patients with acute myocardial infarction.Sci Rep. 2024 Dec 3;14(1):30148. doi: 10.1038/s41598-024-81954-2. Sci Rep. 2024. PMID: 39627297 Free PMC article.
-
Sodium-Glucose Cotransporter-2 Inhibitors After Acute Myocardial Infarction.Biomedicines. 2025 Mar 15;13(3):720. doi: 10.3390/biomedicines13030720. Biomedicines. 2025. PMID: 40149696 Free PMC article. Review.
-
EValuating the Effect of periopeRaTIve empaGliflOzin on cardiac surgery associated acute kidney injury: rationale and design of the VERTIGO study.Clin Kidney J. 2024 Jul 22;17(8):sfae229. doi: 10.1093/ckj/sfae229. eCollection 2024 Aug. Clin Kidney J. 2024. PMID: 39139185 Free PMC article.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Socie. Eur Heart J. 2018;39(2):119–177. doi: 10.1093/eurheartj/ehx393. - DOI - PubMed
-
- Ibanez B, Macaya C, Sánchez-Brunete V, Pizarro G, Fernández-Friera L, Mateos A, et al. Effect of early metoprolol on infarct size in ST-segment–elevation myocardial infarction patients undergoing primary percutaneous coronary intervention. Circulation. 2013;128(14):1495–1503. doi: 10.1161/CIRCULATIONAHA.113.003653. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
