

Medications for opioid use disorder prescribed at hospital discharge associated with decreased opioid agonist dispensing in patients with opioid use disorder requiring critical care: A retrospective study
- PMID: 37778703
- PMCID: PMC10715808
- DOI: 10.1016/j.josat.2023.209176
Medications for opioid use disorder prescribed at hospital discharge associated with decreased opioid agonist dispensing in patients with opioid use disorder requiring critical care: A retrospective study
Abstract
Introduction: Buprenorphine is highly effective for the treatment of opioid use disorder (OUD), and, in recent years, the rates of patients maintained on buprenorphine requiring critical care have been steadily increasing. Currently, no unified guidance exists for buprenorphine management during critical illness. Likewise, we do not know if patients maintained on buprenorphine for OUD are prescribed medications for OUD (MOUD) following hospital discharge or if buprenorphine management influences mu opioid agonist dispensing.
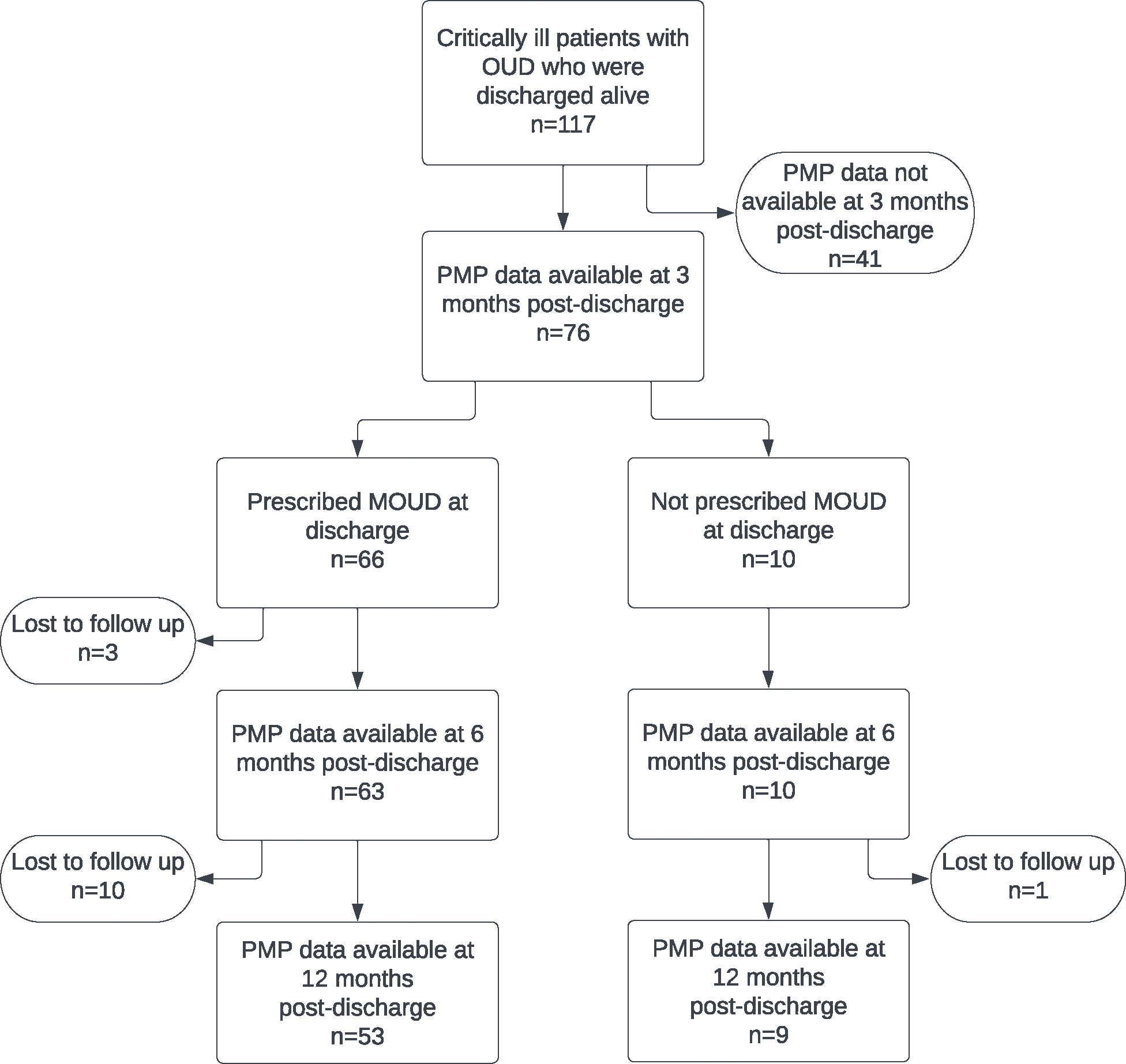
Methods: In our cohort of adults over the age of 18 with OUD, receiving buprenorphine formulations in the 3 months preceding their ICU admission, we sought to investigate the relationship between receipt of MOUD and non-MOUD opioid prescribing up to 12 months following hospital discharge. This was a single-center, retrospective cohort study approved by the MaineHealth institutional review board. The study analyzed differences in prescription rates between discharge and subsequent time points using chi square or Fisher's exact test, as appropriate. We performed analyses using SPSS Statistical Software version 28 (IBM SPSS Inc., Armonk, NY) with significance set at p < 0.05.
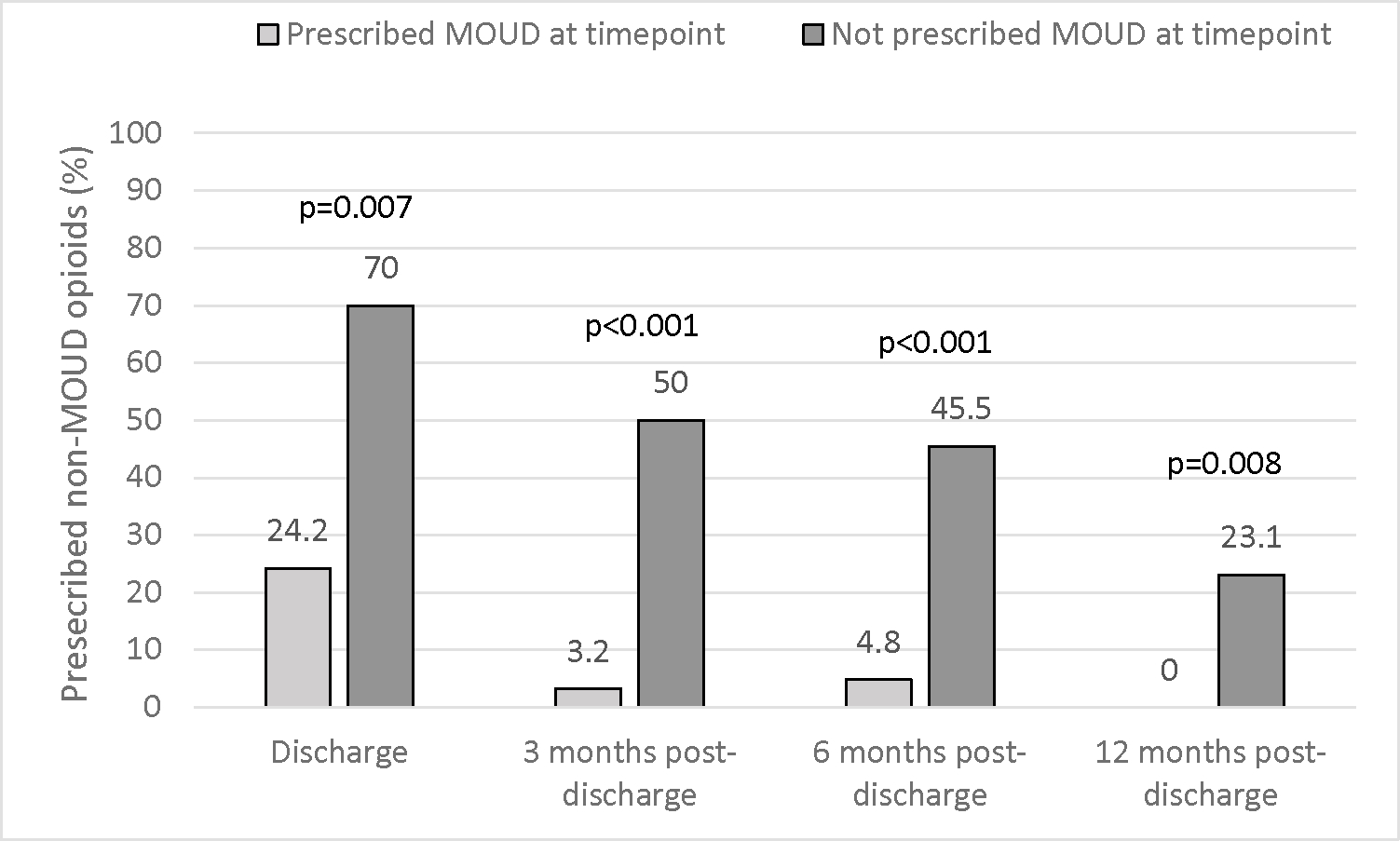
Results: We identified a statistically significant increase in MOUD prescribing 3 months posthospital discharge in patients who received MOUD at time of discharge (87.9 % vs 40 % p = 0.002.) The study found a significant increase in nonbuprenorphine opioid prescribing in patients who did not receive an MOUD prescription at time of discharge (24.2 % vs 70 % p = 0.007). This trend persisted at the 6-month and 12-month time points; however, it did not reach statistical significance. Additionally, the study identified a significant reduction in the incidence of non-MOUD opioid dispensing in patients prescribed MOUD at each time point measured (p = 0.007, p < 0.001. p < 0.001 and p = 0.008 at discharge, 3, 6, and 12 months, respectively).
Conclusions: These findings support continuing buprenorphine dispensing following hospital discharge.
Keywords: Analgesics; Buprenorphine; Intensive care unit; Opioid; Opioid-related disorders.
Copyright © 2023. Published by Elsevier Inc.
Conflict of interest statement
Declaration of competing interest None.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials