

Improving Anemia Assessment in Clinical and Public Health Settings
- PMID: 37778891
- PMCID: PMC11002965
- DOI: 10.1016/j.tjnut.2023.05.032
Improving Anemia Assessment in Clinical and Public Health Settings
Abstract
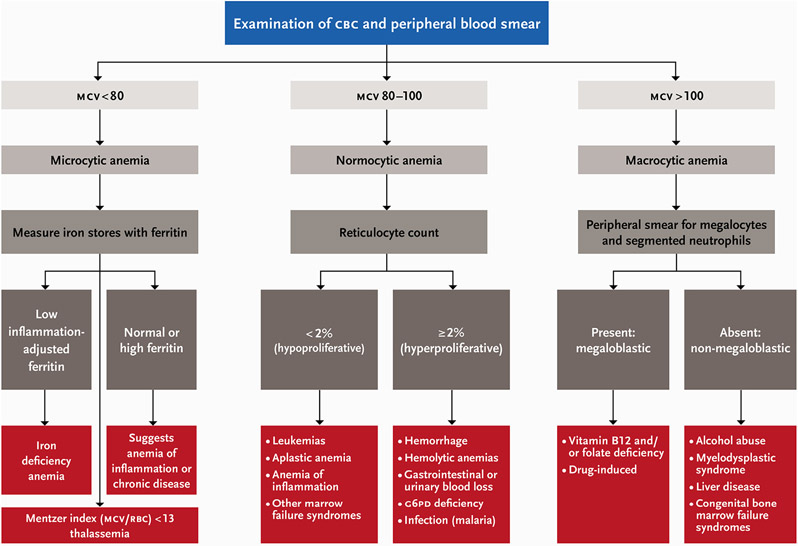
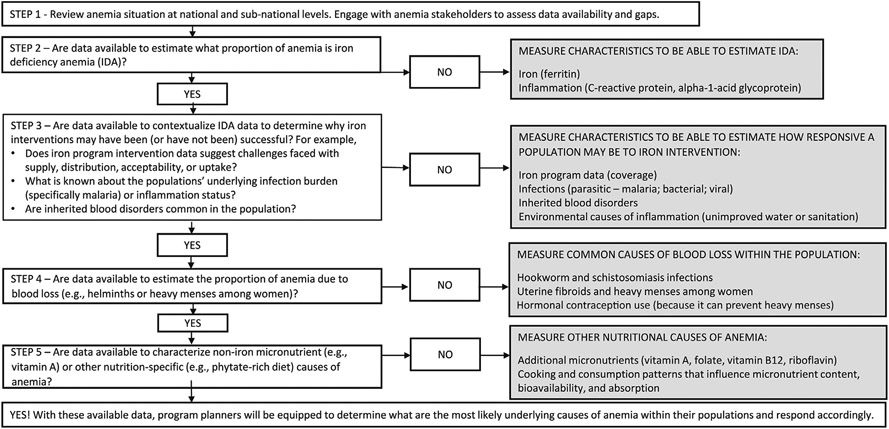
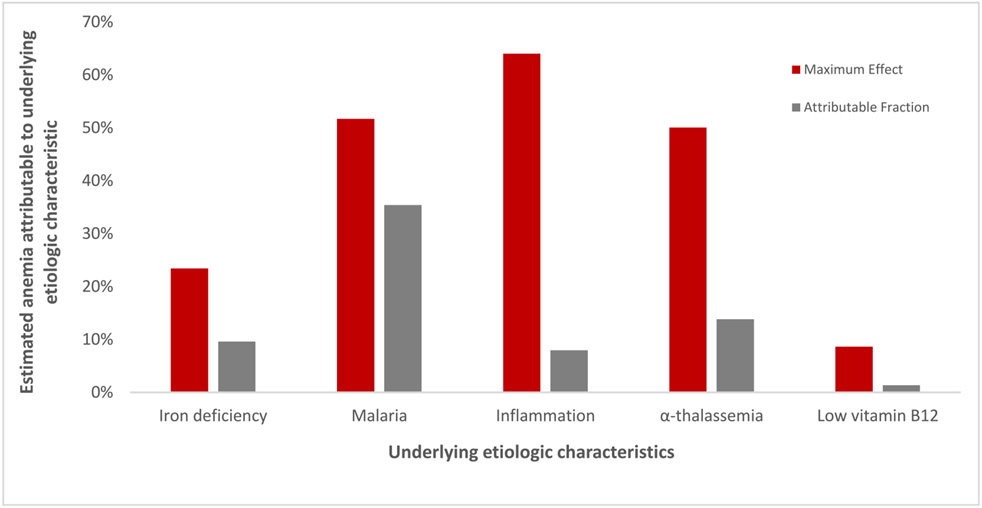
We aim to provide a practical approach to assess anemia and its primary causes, both in clinical settings and in the context of public health programs. Anemia remains a global challenge; thus, to achieve goals for anemia reduction and assess progress, standardized approaches are required for the assessment of anemia and its causes. We first provide a brief review of how to assess anemia, based on hemoglobin concentrations and cutoffs that correspond to age, sex, and physiologic status. Next, we discuss how to assess the likely causes of anemia in different settings. The causes of anemia are classified as non-nutritional (for example, because of infection, inflammation, blood loss, or genetic disorders) or nutrition-specific (for example, because of deficiencies of iron, vitamin A, riboflavin, vitamin B12, or folate). There is an important overlap between these 2 categories, such as the increased likelihood of iron deficiency in the context of inflammation. Given the multifaceted nature of anemia etiology, we introduce a framework for anemia assessment based on the "ecology of anemia," which recognizes its many overlapping causes. This conceptual framework is meant to inform what data on anemia causes may need to be collected in population surveys. The framework has a supporting table with information on the diagnostic tests, biomarkers and proposed cutoffs, characteristics, and feasibility of collecting the myriad information that can help elucidate the anemia etiology. We also provide examples of how this framework can be applied to interpret the anemia risk factor data from population-based surveys that can inform decisions about context-specific interventions. Finally, we present research gaps and priorities related to anemia assessment.
Keywords: anemia assessment; anemia etiology; hemoglobin; population-based methods.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest
PS reports a relationship with Bill & Melinda Gates Foundation that includes: funding and grants. KB reports a relationship with Micronutrient Forum that includes: board membership. KB reports a relationship with Bill & Melinda Gates Foundation that includes: consulting or advisory. KB reports relationships with Nutrition International and the Bill & Melinda Gates Foundation that includes: funding and grants. All other authors report no conflicts of interest.
Figures
References
-
- Bond MM, Richards-Kortum RR, Drop-to-drop variation in the cellular components of fingerprick blood: Implications for point-of-care diagnostic development, Am. J. Clin. Pathol 144 (2015) 885–894. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
