

Liver Inclusion Appears to Be Protective Against Graft Loss-Due-to Chronic But Not Acute Rejection Following Intestinal Transplantation
- PMID: 37779512
- PMCID: PMC10538304
- DOI: 10.3389/ti.2023.11568
Liver Inclusion Appears to Be Protective Against Graft Loss-Due-to Chronic But Not Acute Rejection Following Intestinal Transplantation
Abstract
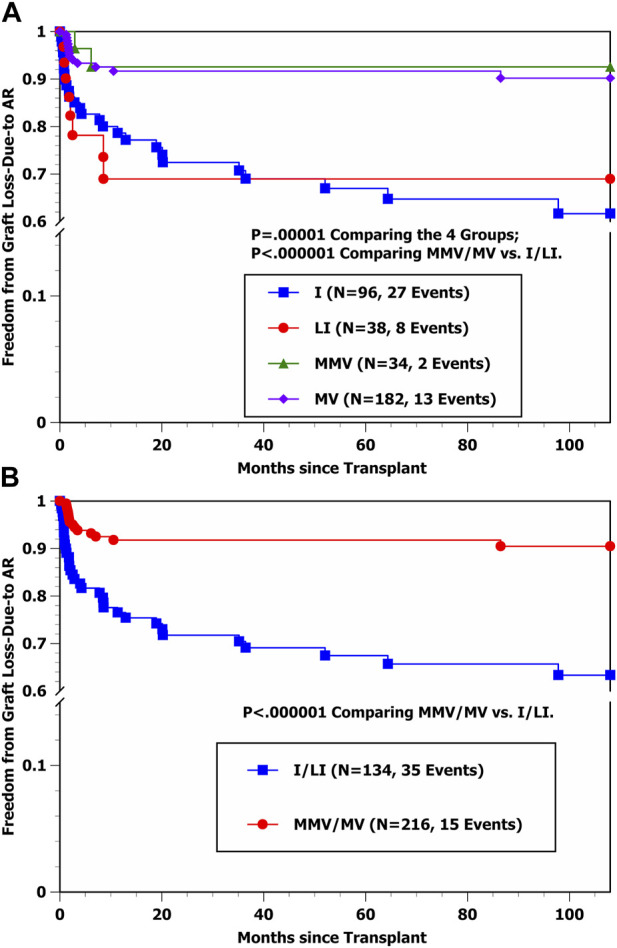
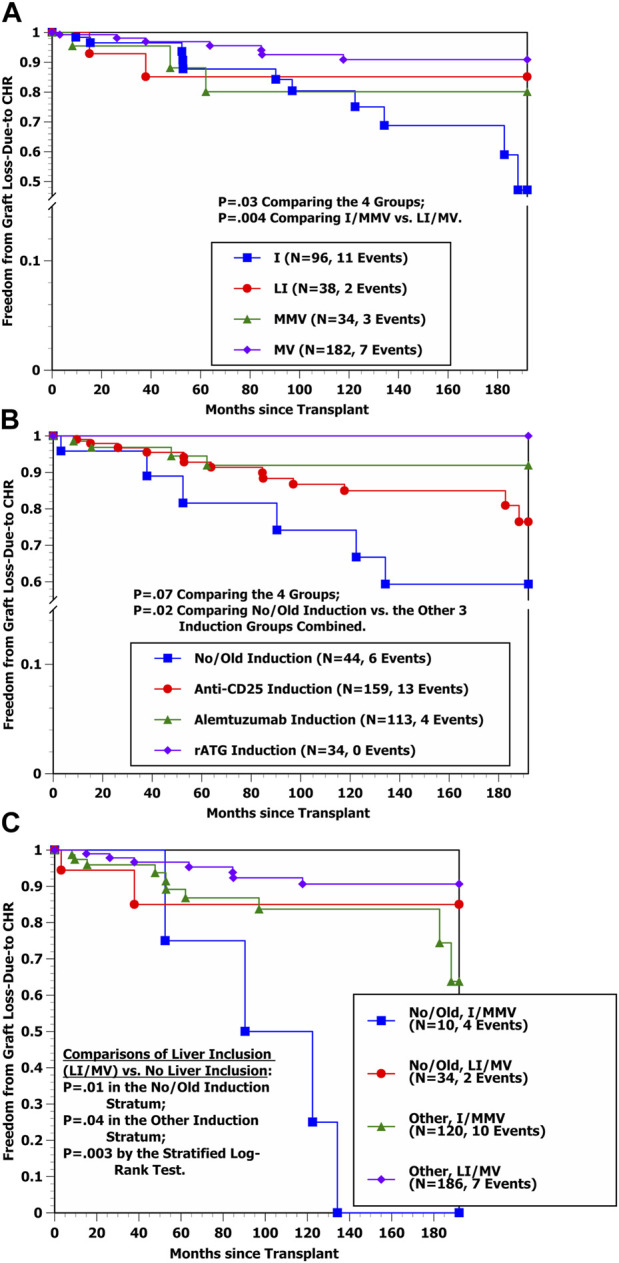
In intestinal transplantation, while other centers have shown that liver-including allografts have significantly more favorable graft survival and graft loss-due-to chronic rejection (CHR) rates, our center has consistently shown that modified multivisceral (MMV) and full multivisceral (MV) allografts have significantly more favorable acute cellular rejection (ACR) and severe ACR rates compared with isolated intestine (I) and liver-intestine (LI) allografts. In the attempt to resolve this apparent discrepancy, we performed stepwise Cox multivariable analyses of the hazard rates of developing graft loss-due-to acute rejection (AR) vs. CHR among 350 consecutive intestinal transplants at our center with long-term follow-up (median: 13.5 years post-transplant). Observed percentages developing graft loss-due-to AR and CHR were 14.3% (50/350) and 6.6% (23/350), respectively. Only one baseline variable was selected into the Cox model indicating a significantly lower hazard rate of developing graft loss-due-to AR: Transplant Type MMV or MV (p < 0.000001). Conversely, two baseline variables were selected into the Cox model indicating a significantly lower hazard rate of developing graft loss-due-to CHR: Received Donor Liver (LI or MV) (p = 0.002) and Received Induction (p = 0.007). In summary, while MMV/MV transplants (who receive extensive native lymphoid tissue removal) offered protection against graft loss-due-to AR, liver-containing grafts appeared to offer protection against graft loss-due-to CHR, supporting the results of other studies.
Keywords: chronic rejection; graft loss-due-to acute rejection; graft loss-due-to chronic rejection; intestinal transplantation; long-term results CHR; prognostic factors.
Copyright © 2023 Vianna, Gaynor, Selvaggi, Farag, Garcia, Tekin, Tabbara and Ciancio.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials