

Systemic juvenile idiopathic arthritis: The Great Ormond Street Hospital experience (2005-2021)
- PMID: 37780048
- PMCID: PMC10536248
- DOI: 10.3389/fped.2023.1218312
Systemic juvenile idiopathic arthritis: The Great Ormond Street Hospital experience (2005-2021)
Abstract
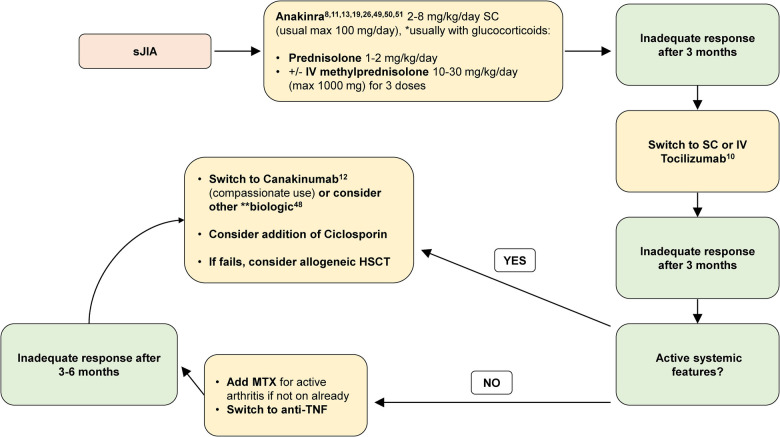
Systemic juvenile idiopathic arthritis (sJIA) is a complex, systemic inflammatory disorder driven by both innate and adaptive immunity. Improved understanding of sJIA pathophysiology has led to recent therapeutic advances including a growing evidence base for the earlier use of IL-1 or IL-6 blockade as first-line treatment. We conducted a retrospective case notes review of patients diagnosed with sJIA over a 16-year period (October 2005-October 2021) at Great Ormond Street Hospital for Children. We describe the clinical presentation, therapeutic interventions, complications, and remission rates at different timepoints over the disease course. We examined our data, which spanned a period of changing therapeutic landscape, to try and identify potential therapeutic signals in patients who received biologic treatment early in the disease course compared to those who did not. A total of 76-children (female n = 40, 53%) were diagnosed with sJIA, median age 4.5 years (range 0.6-14.1); 36% (27/76) presented with suspected or confirmed macrophage activation syndrome. A biologic disease-modifying anti-rheumatic drug (bDMARD) alone was commenced as first-line treatment in 28% (n = 21/76) of the cohort; however, at last review, 84% (n = 64/76) had received treatment with a bDMARD. Clinically inactive disease (CID) was achieved by 88% (n = 67/76) of the cohort at last review; however, only 32% (24/76) achieved treatment-free CID. At 1-year follow-up, CID was achieved in a significantly greater proportion of children who received treatment with a bDMARD within 3 months of diagnosis compared to those who did not (90% vs. 53%, p = 0.002). Based on an ever-increasing evidence base for the earlier use of bDMARD in sJIA and our experience of the largest UK single-centre case series described to date, we now propose a new therapeutic pathway for children diagnosed with sJIA in the UK based on early use of bDMARDs. Reappraisal of the current National Health Service commissioning pathway for sJIA is now urgently required.
Keywords: IL-1 blockade; IL-6 blocking; Still’s disease; biologic; systemic JIA.
© 2023 Foley, McKenna, Gallagher, McLellan, Alkhdher, Lacassagne, Moraitis, Papadopoulou, Pilkington, Al Obaidi, Eleftheriou and Brogan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton 2001. J Rheumatol. (2004) 31:390–2. - PubMed
-
- Silva JR, Brito I. Systemic juvenile idiopathic arthritis versus adult-onset Still’s disease: the pertinence of changing the current classification criteria. Acta Reum Port. (2020) 45:150–1. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources