

Effectiveness and potential mechanism of Jiawei-Xiaoyao-San for hyperthyroidism: a systematic review
- PMID: 37780612
- PMCID: PMC10534980
- DOI: 10.3389/fendo.2023.1241962
Effectiveness and potential mechanism of Jiawei-Xiaoyao-San for hyperthyroidism: a systematic review
Abstract
Objectives: To evaluate the effectiveness and potential mechanism of traditional Chinese medicine Jiawei-Xiaoyao-San (JWXYS) as an adjunct or mono- therapy for antithyroid drugs (ATDs) in the treatment of hyperthyroidism.
Methods: Eight databases and three trial registries were searched from inception until May 2023. Randomized controlled trials (RCTs) were included and meta-analysis was conducted using RevMan 5.4 and Stata 14.0. The Cochrane risk of bias (ROB) tool 1.0 and GRADE tool was used for quality appraisal. The findings from case reports using mono-JWXYS and pharmacological studies were summarized in tables.
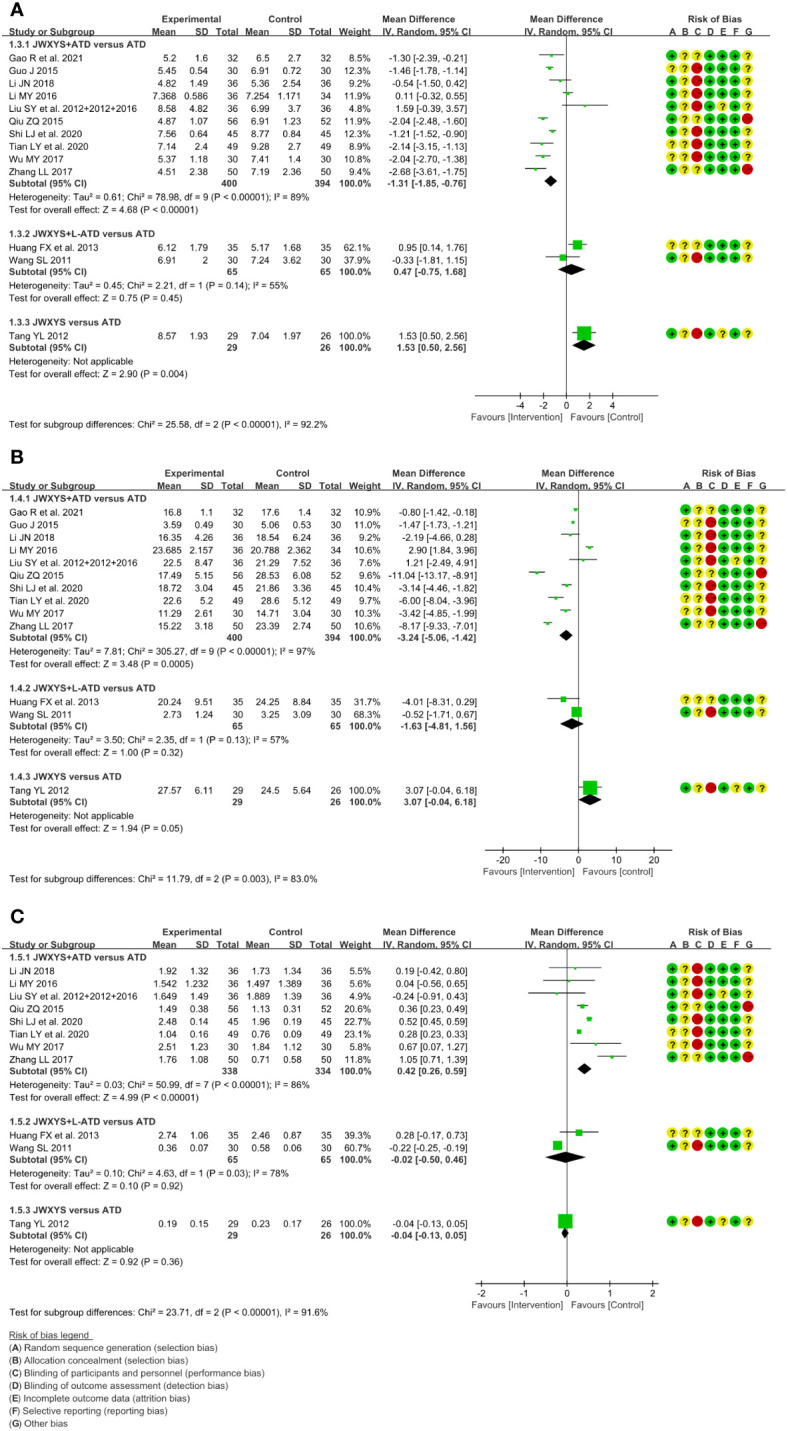
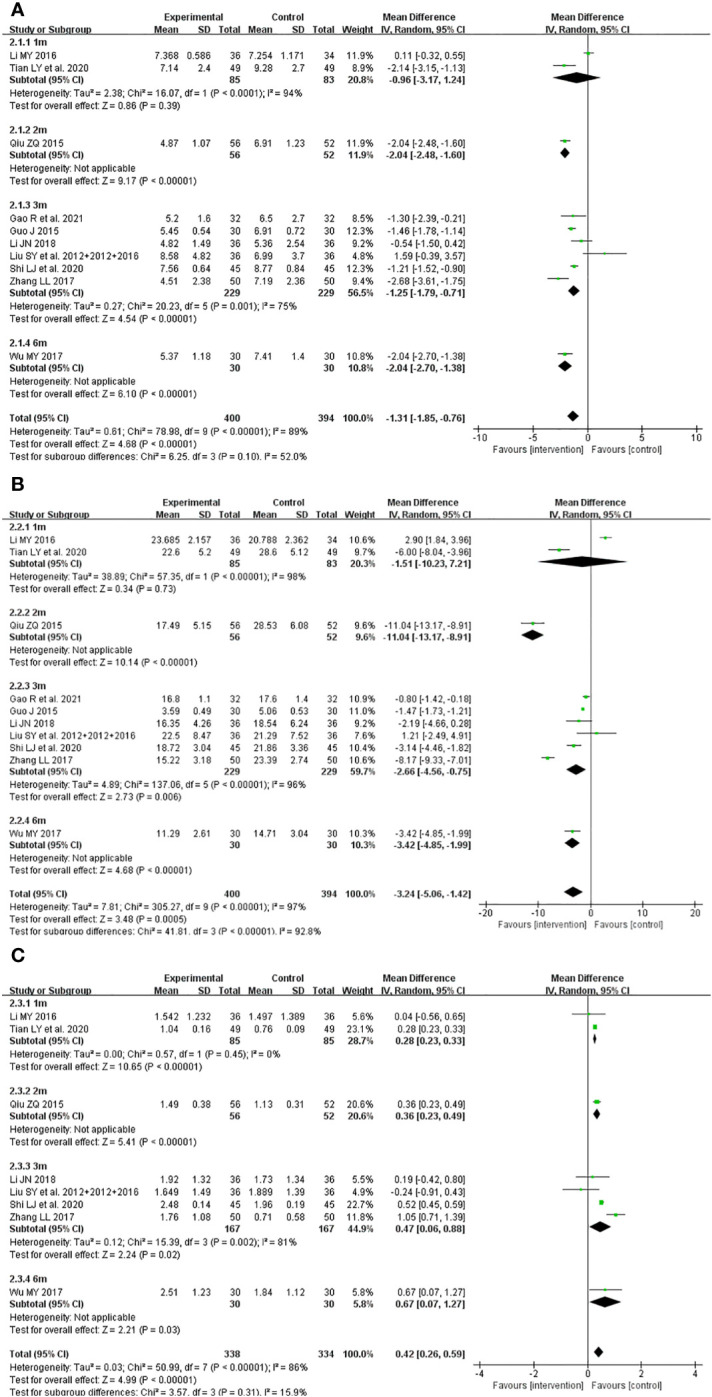
Results: Thirteen RCTs with 979 participants were included. The majority of the included studies were assessed as high risk of bias in one ROB domain. Compared with ATDs, JWXYS plus ATDs resulted in lower free triiodothyronine (FT3) (MD = -1.31 pmol/L, 95% CI [-1.85, -0.76]; low-certainty), lower free thyroxine (MD = -3.24 pmol/L, 95% CI [-5.06, -1.42]; low-certainty), higher thyroid stimulating hormone (MD = 0.42 mIU/L, 95% CI [0.26, 0.59]; low-certainty), higher effectiveness rate of traditional Chinese medicine syndrome (RR = 1.28, 95% CI [1.08, 1.52]; low-certainty), lower goiter score (MD = -0.66, 95% CI [-1.04, -0.29]; very low-certainty), lower thyrotrophin receptor antibody (SMD = -0.44, 95% CI [-0.73, -0.16]; low-certainty) and fewer adverse events (AEs) (RR = 0.34, 95% CI [0.18, 0.67]; moderate-certainty). Compared with regular dosage of ATDs, JWXYS plus half-dose ATDs resulted in fewer AEs (RR = 0.24, 95% CI [0.10, 0.59]; low-certainty). Compared with ATDs in 1 trial, JWXYS resulted in higher FT3, lower goiter score and fewer AEs. Three case reports showed that the reasons patients sought TCM-only treatment include severe AEs and multiple relapses. Three pharmacological studies demonstrated that JWXYS restored Th17/Treg balance, lowered deiodinases activity, regulated thyroid cell proliferation and apoptosis, and alleviated liver oxidative stress in mouse or rat models.
Conclusion: JWXYS may enhance the effectiveness of ATDs for hyperthyroidism, particularly in relieving symptoms and reducing AEs. Mono-JWXYS is not recommended except in patients intolerant to ATDs. The findings should be interpreted with caution due to overall high risk of bias. Further pharmacological studies with more reliable models are needed.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42023394923.
Keywords: Jiawei-Xiaoyao-San; hyperthyroidism; meta-analysis; pharmacological studies; randomized controlled trials; systematic review; traditional Chinese medicine.
Copyright © 2023 Ma, Zhang, Zhao, Tang, Zhu, Liu, Xu, Wang, Peng, Liu and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures








Similar articles
-
Efficacy and safety of Prunella vulgaris L. combined with antithyroid drugs for hyperthyroidism: a systematic review and meta-analysis.Front Pharmacol. 2025 Feb 27;16:1530152. doi: 10.3389/fphar.2025.1530152. eCollection 2025. Front Pharmacol. 2025. PMID: 40083379 Free PMC article.
-
Efficacy and safety of Danggui Liuhuang Decoction combined with antithyroid drugs for hyperthyroidism: A systematic review and meta-analysis.J Ethnopharmacol. 2025 Feb 11;341:119253. doi: 10.1016/j.jep.2024.119253. Epub 2024 Dec 26. J Ethnopharmacol. 2025. PMID: 39732298
-
Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: a living systematic review.Cochrane Database Syst Rev. 2020 Oct 12;10:CD013600. doi: 10.1002/14651858.CD013600.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 May 20;5:CD013600. doi: 10.1002/14651858.CD013600.pub4. PMID: 33044747 Updated.
-
External therapy of traditional Chinese medicine for treating irritable bowel syndrome with diarrhea: A systematic review and meta-analysis.Front Med (Lausanne). 2022 Aug 9;9:940328. doi: 10.3389/fmed.2022.940328. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36017012 Free PMC article.
-
Acupuncture and related interventions for the treatment of symptoms associated with carpal tunnel syndrome.Cochrane Database Syst Rev. 2018 Dec 2;12(12):CD011215. doi: 10.1002/14651858.CD011215.pub2. Cochrane Database Syst Rev. 2018. PMID: 30521680 Free PMC article.
Cited by
-
Efficacy and safety of Prunella vulgaris L. combined with antithyroid drugs for hyperthyroidism: a systematic review and meta-analysis.Front Pharmacol. 2025 Feb 27;16:1530152. doi: 10.3389/fphar.2025.1530152. eCollection 2025. Front Pharmacol. 2025. PMID: 40083379 Free PMC article.
-
The Combined Treatment of Chinese Herbal Medicines Is Correlated with a Lower Risk of Rheumatoid Arthritis in Patients with Depression: Evidence from a Population-Based Patient-Control Study.Pharmaceuticals (Basel). 2025 Mar 27;18(4):480. doi: 10.3390/ph18040480. Pharmaceuticals (Basel). 2025. PMID: 40283919 Free PMC article.
-
Efficacy of Xiaoyao-san preparations in treating Hashimoto's thyroiditis: a meta-analysis and systematic review.Front Pharmacol. 2025 Jun 13;16:1528506. doi: 10.3389/fphar.2025.1528506. eCollection 2025. Front Pharmacol. 2025. PMID: 40584613 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical