

Techniques and Tips to Arthroscopically Remove Prominent and Loose Shoulder Joint Hardware
- PMID: 37780655
- PMCID: PMC10533940
- DOI: 10.1016/j.eats.2023.04.031
Techniques and Tips to Arthroscopically Remove Prominent and Loose Shoulder Joint Hardware
Abstract
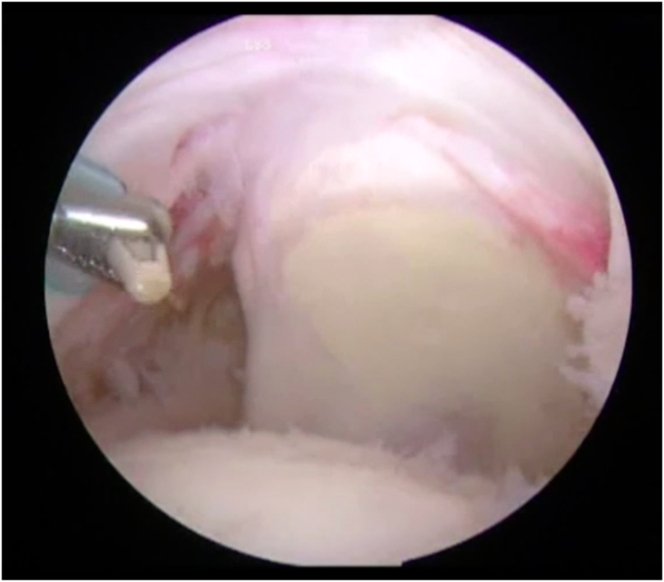
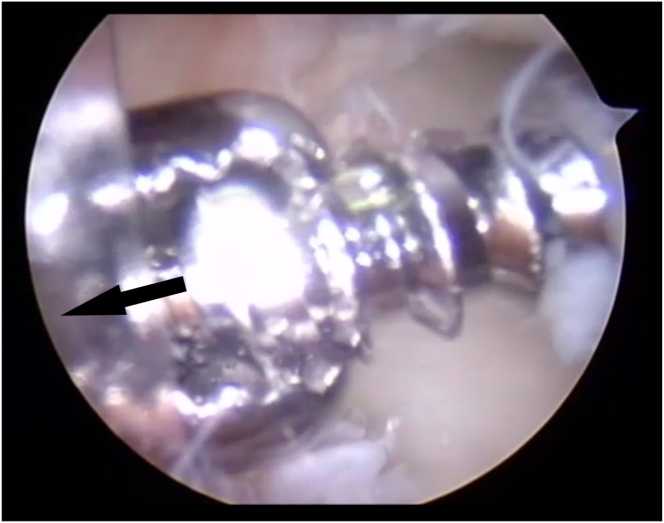
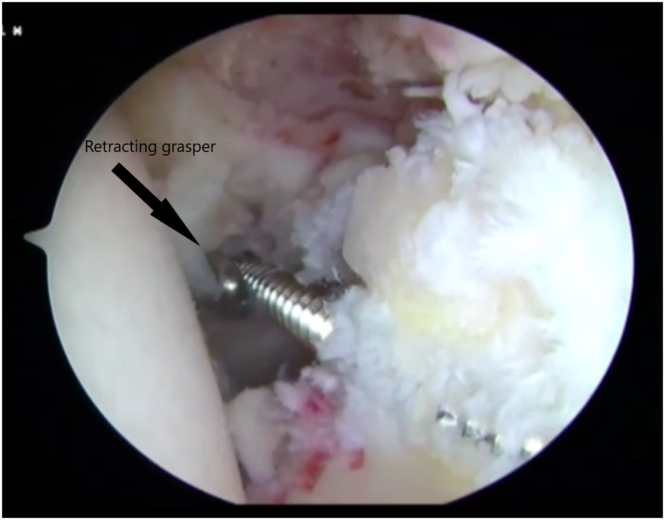
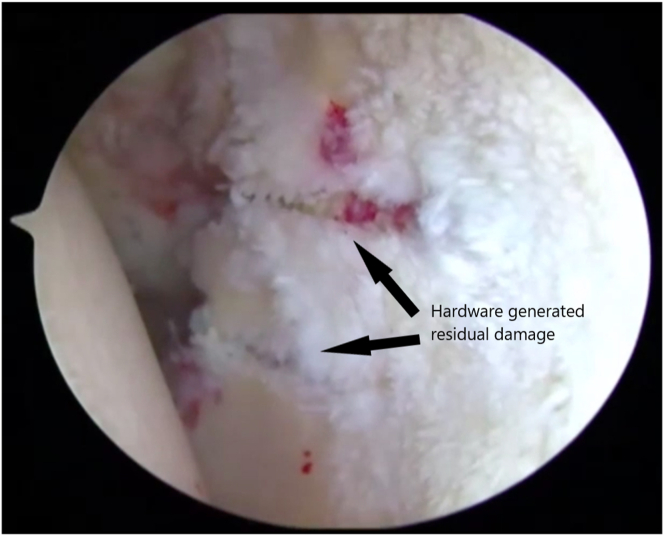
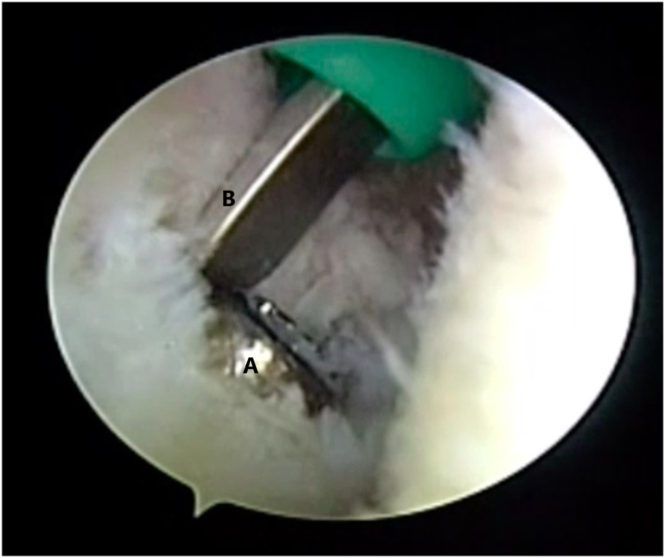
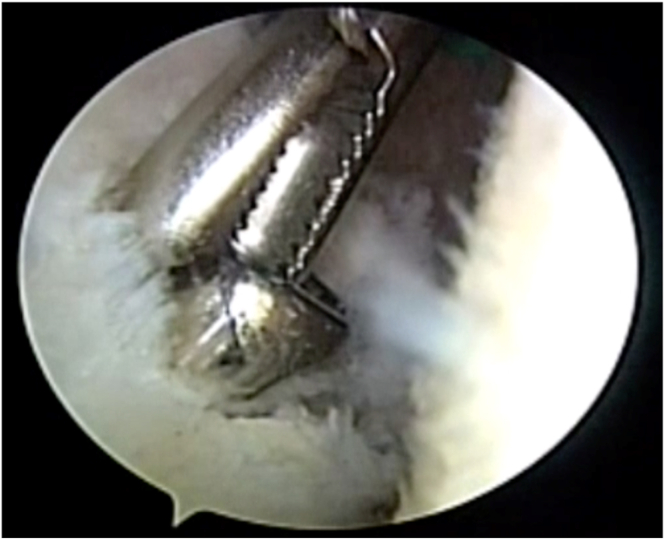
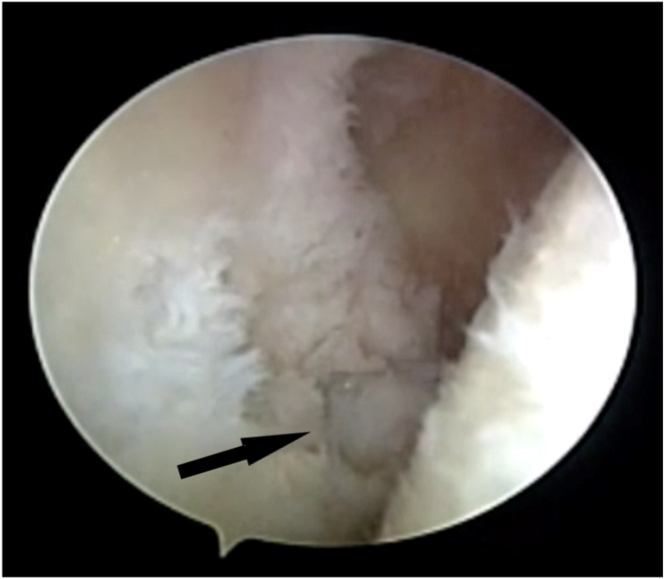
The number of arthroscopic shoulder operations has continued to steadily increase in recent years, with a projection of over 500,000 rotator cuff operations in 2023. Although the incidence of anchor pullout, hardware failure, and aberrant hardware placement is relatively low, this increased volume of shoulder operations has inevitably resulted in a consequent increase in the number of patients who experience such hardware complications. These hardware issues can cause significant pain, limit shoulder function, and cause permanent damage to the shoulder articular cartilage. The described arthroscopic techniques are presented to provide tools and strategies to safely and effectively remove prominent and loose shoulder joint hardware.
© 2023 The Authors.
Figures


Similar articles
-
Novel and reproducible technique coping with intraoperative anchor pullout during arthroscopic rotator cuff repair.Knee Surg Sports Traumatol Arthrosc. 2021 Jan;29(1):223-229. doi: 10.1007/s00167-020-05935-4. Epub 2020 Mar 30. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32232537
-
Glenoid damage from articular protrusion of metal suture anchor after arthroscopic rotator cuff repair.Am J Orthop (Belle Mead NJ). 2015 Mar;44(3):E78-80. Am J Orthop (Belle Mead NJ). 2015. PMID: 25750956
-
Midterm outcomes of arthroscopic rotator cuff repair in patients aged 75 years and older.J Shoulder Elbow Surg. 2020 Jul;29(7S):S17-S22. doi: 10.1016/j.jse.2019.11.022. Epub 2020 Feb 19. J Shoulder Elbow Surg. 2020. PMID: 32088076
-
Risk Factors and Corresponding Management for Suture Anchor Pullout during Arthroscopic Rotator Cuff Repair.J Clin Med. 2022 Nov 21;11(22):6870. doi: 10.3390/jcm11226870. J Clin Med. 2022. PMID: 36431347 Free PMC article. Review.
-
Repair of the rotator cuff. Mini-open and arthroscopic repairs.Clin Sports Med. 2000 Jan;19(1):77-99. doi: 10.1016/s0278-5919(05)70297-0. Clin Sports Med. 2000. PMID: 10652666 Review.
Cited by
-
Humeral Head Articular Cartilage Damage by a Retained Arthroscopic Suture Anchor Inserter in a College Athlete.Cureus. 2023 Sep 1;15(9):e44536. doi: 10.7759/cureus.44536. eCollection 2023 Sep. Cureus. 2023. PMID: 37790009 Free PMC article.
References
-
- Ma R., Chow R., Choi L., Diduch D. Arthroscopic rotator cuff repair: Suture anchor properties, modes of failure and technical considerations. Expert Rev Med Devices. 2011;8:377–387. - PubMed
-
- iData Research Over 460,000 rotator cuff surgeries per year reported in the United States by iData Research. https://idataresearch.com/over-460000-rotator-cuff-surgeries-per-year-re... Published April 7, 2018.
-
- Benson E.C., MacDermid J.C., Drosdowech D.S., Athwal G.S. The incidence of early metallic suture anchor pullout after arthroscopic rotator cuff repair. Arthroscopy. 2010;26:310–315. - PubMed
-
- Skaliczki G., Paladini P., Merolla G., Campi F., Porcellini G. Early anchor displacement after arthroscopic rotator cuff repair. Int Orthop. 2015;39:915–920. - PubMed
LinkOut - more resources
Full Text Sources
