

High tibial lateral closing wedge and opening wedge valgus osteotomy produce different effects on posterior tibial slope and patellar height
- PMID: 37780911
- PMCID: PMC10536261
- DOI: 10.3389/fsurg.2023.1219614
High tibial lateral closing wedge and opening wedge valgus osteotomy produce different effects on posterior tibial slope and patellar height
Abstract
Objective: To compare the clinical outcomes of performing a closed tibial high osteotomy with an open osteotomy and the changes in posterior tibia slope and patellar height.
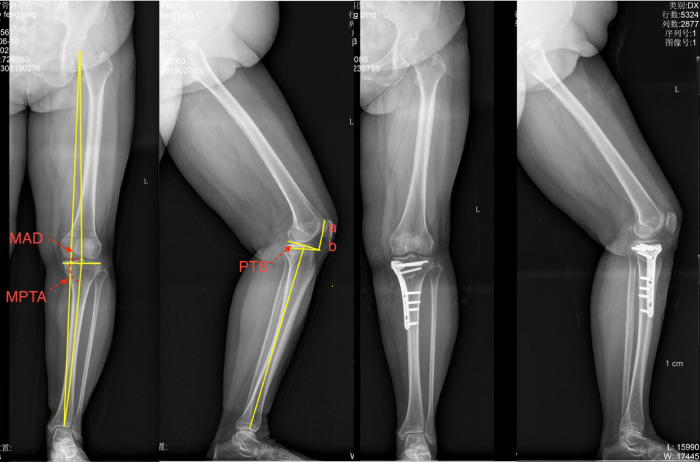
Methods: Methods were collected from three hundred and forty patients (440 knees) with high tibial osteotomy performed from January 2019 to January 2020. Forty patients (50 knees) had a lateral closed wedge tibial osteotomy (LCWHTO), and 300 patients (390 knees) had a medial open wedge tibial osteotomy (MOWHTO). The follow-up periods were 20.5 months and 19.9 months, respectively. At the final follow-up visit, both groups evaluated the Lysholm score and joint range of motion (ROM). Changes in preoperative and postoperative mechanical axis deviation (MAD), proximal medial tibial angle (MPTA), posterior tibial slope (PTS), and M-K index were compared between the two groups of patients.
Results: Lysholm scores were 79.6 ± 15.6 preoperatively and 96.0 ± 5.0 postoperatively in the LCWHTO group (p < 0.01); 83.7 ± 16.0 preoperatively and 94.3 ± 9.1 postoperatively in the MOWHTO group (p < 0.01). ROM was 136.0° ± 8.4° preoperatively and 133.2° ± 10.1° postoperatively in the LCWHTO group (p > 0.05); 136.5° ± 8.4° preoperatively and 135.7° ± 9.3° postoperatively in the MOWHTO group (p > 0.05). the MAD was (26.5 ± 4.1) mm preoperatively and 0.3 ± 2.9 mm postoperatively in the LCWHTO group (p < 0.01); 21.8 ± 6.5 mm preoperatively and -0.3 ± 2.6 mm postoperatively in the MOWHTO group (p < 0.01). The MPTA in the LCWHTO group was 75.3° ± 3.2° preoperatively and 89.5° ± 2.4° postoperatively (p < 0.01). 77.1° ± 3.0° preoperatively and 90.6° ± 2.7° postoperatively in the MOWHTO group (p < 0.01). M-K index was 0.78 ± 0.08 preoperatively and 0.79 ± 0.07 postoperatively in the LCWHTO group (p > 0.05). 0.78 ± 0.05 before and 0.75 ± 0.05 after surgery in the MOWHTO. 10.8° ± 3.0° PTS before and 8.1° ± 3.4° after surgery in the LCWHTO group (p < 0.05); 10.2° ± 3.1° preoperatively and 10.9° ± 4.0° postoperatively (p > 0.05).
Conclusions: LCWHTO decreases the PTS and has no effect on patellar height; MOWHTO does not affect the PTS but decreases patellar height. The patient should individualize the choice of the osteotomy.
Keywords: closed; high tibial osteotomy (HTO); open; patellar height (PH); posterior tibial slope (PTS).
© 2023 Ji, Gao, Zhang, Pan, Zhu, Jiang and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Patellar height and posterior tibial slope after open- and closed-wedge high tibial osteotomy: a radiological study on 100 patients.Am J Sports Med. 2010 Feb;38(2):323-9. doi: 10.1177/0363546509348050. Epub 2009 Dec 31. Am J Sports Med. 2010. PMID: 20044496
-
Patellar height and tibial slope after opening-wedge proximal tibial osteotomy: a prospective study.Am J Sports Med. 2010 Jan;38(1):160-70. doi: 10.1177/0363546509342701. Epub 2009 Sep 18. Am J Sports Med. 2010. PMID: 19767536
-
Maintaining Posterior Tibial Slope and Patellar Height During Medial Opening Wedge High Tibial Osteotomy.Orthop J Sports Med. 2023 Dec 11;11(12):23259671231213595. doi: 10.1177/23259671231213595. eCollection 2023 Dec. Orthop J Sports Med. 2023. PMID: 38090657 Free PMC article.
-
Bone Healing and Clinical Outcome Following Medial Opening-wedge High Tibial Osteotomy Using Wedge-Shaped Cancellous Allograft.Orthop Surg. 2024 Jan;16(1):86-93. doi: 10.1111/os.13939. Epub 2023 Nov 28. Orthop Surg. 2024. PMID: 38014470 Free PMC article.
-
A Systematic Review on Selected Complications of Open-Wedge High Tibial Osteotomy from Clinical and Biomechanical Perspectives.Appl Bionics Biomech. 2021 Oct 31;2021:9974666. doi: 10.1155/2021/9974666. eCollection 2021. Appl Bionics Biomech. 2021. PMID: 34754331 Free PMC article. Review.
Cited by
-
Comparative biomechanical analysis of tibial posterior slope in medial open wedge high tibial osteotomy vs. distal tuberosity osteotomy with and without anterior-posterior screw: a study using porcine tibia.SICOT J. 2024;10:41. doi: 10.1051/sicotj/2024042. Epub 2024 Oct 21. SICOT J. 2024. PMID: 39431748 Free PMC article.
-
Changes in Patellar Height and Tibial Posterior Slope after Biplanar High Tibial Osteotomy with Computer-Designed Personalized Surgical Guides: A Retrospective Study.Orthop Surg. 2024 May;16(5):1143-1152. doi: 10.1111/os.14049. Epub 2024 Apr 1. Orthop Surg. 2024. PMID: 38561920 Free PMC article.
-
Maintaining Posterior Tibial Slope and Patellar Height During Medial Opening Wedge High Tibial Osteotomy: Response.Orthop J Sports Med. 2024 Oct 31;12(10):23259671241270306. doi: 10.1177/23259671241270306. eCollection 2024 Oct. Orthop J Sports Med. 2024. PMID: 39492873 Free PMC article. No abstract available.
-
Maintaining Posterior Tibial Slope and Patellar Height During Medial Opening Wedge High Tibial Osteotomy: Letter to the Editor.Orthop J Sports Med. 2024 Oct 31;12(10):23259671241270307. doi: 10.1177/23259671241270307. eCollection 2024 Oct. Orthop J Sports Med. 2024. PMID: 39493595 Free PMC article. No abstract available.
-
Comparative impact of high tibial osteotomy and supramalleolar osteotomy on limb alignment and ankle function: a retrospective study.J Orthop Surg Res. 2025 Mar 4;20(1):234. doi: 10.1186/s13018-025-05511-x. J Orthop Surg Res. 2025. PMID: 40038785 Free PMC article.
References
LinkOut - more resources
Full Text Sources