

Chronic rhinosinusitis with nasal polyps and allergic rhinitis as different multimorbid treatable traits in asthma
- PMID: 37781668
- PMCID: PMC10510007
- DOI: 10.1016/j.jacig.2023.100134
Chronic rhinosinusitis with nasal polyps and allergic rhinitis as different multimorbid treatable traits in asthma
Abstract
Background: Respiratory multimorbidities are linked to asthma, such as allergic rhinitis (AR) with early allergic asthma and chronic rhinosinusitis (CRS) with nasal polyps (CRSwNP) with late nonallergic asthma.
Objective: Our aim was to investigate the association of asthma severity and control with specific upper airway phenotypes.
Method: Patients with asthma were prospectively recruited from 23 pulmonology and ear, nose, and throat clinics. Asthma severity and control, as well as upper airway comorbidities (AR and non-AR [NAR], CRSwNP, and CRS without nasal polyps [CRSsNP]) were assessed according to international consensus guidelines definitions.
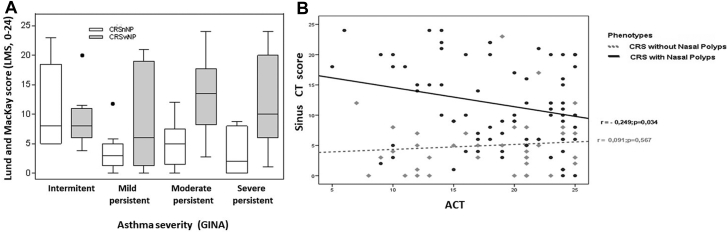
Results: A total of 492 asthmatic patients were included. Half of the asthmatic patients (49.6%) had associated rhinitis (37.0% had AR and 12.6% had NAR) and 36.2% had CRS (16.7% had CRSsNP and 19.5% had CRSwNP), whereas 14.2% had no sinonasal symptoms. Most cases of AR (78%) and NAR (84%) were present in patients with mild-to-moderate asthma, whereas CRSwNP was more frequent in patients with severe asthma (35% [P < .001]), mainly nonatopic asthma (44% [P < .001]). Patients with severe asthma with CRSwNP had worse asthma control, which was correlated (r = 0.249 [P = .034]) with sinus occupancy. Multiple logistic regression analysis showed that late-onset asthma, intolerance of aspirin and/or nonsteroidal anti-inflammatory drugs, and CRSwNP were independently associated with severe asthma.
Conclusion: Severe asthma is associated with CRSwNP, with sinus occupancy affecting asthma control. This study has identified 2 main different upper airway treatable traits, AR and CRSwNP, which need further evaluation to improve management and control of patients with asthma.
Keywords: Asthma; allergic rhinitis; asthma control; asthma severity; chronic rhinosinusitis with nasal polyps; united airway disease.
© 2023 Merck Sharp & Dohme LLC., a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, The Author(s).
Figures




References
-
- Bousquet J., Khaltaev N., Cruz A., Yorgancioglu A., Chuchalin A. International European Respiratory Society/American Thoracic Society guidelines on severe asthma. Eur Respir J. 2014;44:1377–1378. - PubMed
-
- Vennera M. del C., Picado C., Herráez L., Galera J., Casafont J., Study Group CONTROL Factors associated with severe uncontrolled asthma and the perception of control by physicians and patients. Arch Bronconeumol. 2014;50:384–391. - PubMed
-
- Yii A.C.A., Tay T.R., Choo X.N., Koh M.S.Y., Tee A.K.H., Wang D.Y. Precision medicine in united airways disease: a “treatable traits” approach. Allergy. 2018;73:1964–1978. - PubMed
-
- Jarvis D., Newson R., Lotvall J., Hastan D., Tomansen P., Keil T., et al. Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy. 2012;67:91–98. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
