

Epidemiology of Trauma-Related Hemorrhage and Time to Definitive Care Across North America: Making the Case for Bleeding Control Education
- PMID: 37781932
- PMCID: PMC10694464
- DOI: 10.1017/S1049023X23006428
Epidemiology of Trauma-Related Hemorrhage and Time to Definitive Care Across North America: Making the Case for Bleeding Control Education
Abstract
Introduction: Uncontrolled trauma-related hemorrhage remains the primary preventable cause of death among those with critical injury.
Study objective: The purpose of this investigation was to evaluate the types of trauma associated with critical injury and trauma-related hemorrhage, and to determine the time to definitive care among patients treated at major trauma centers who were predicted to require massive transfusion.
Methods: A secondary analysis was performed of the Pragmatic, Randomized, Optimal Platelet and Plasma Ratios (PROPPR) trial data (N = 680). All patients included were predicted to require massive transfusion and admitted to one of 12 North American trauma centers. Descriptive statistics were used to characterize patients, including demographics, type and mechanism of injury, source of bleeding, and receipt of prehospital interventions. Patient time to definitive care was determined using the time from activation of emergency services to responder arrival on scene, and time from scene departure to emergency department (ED) arrival. Each interval was calculated and then summed for a total time to definitive care.
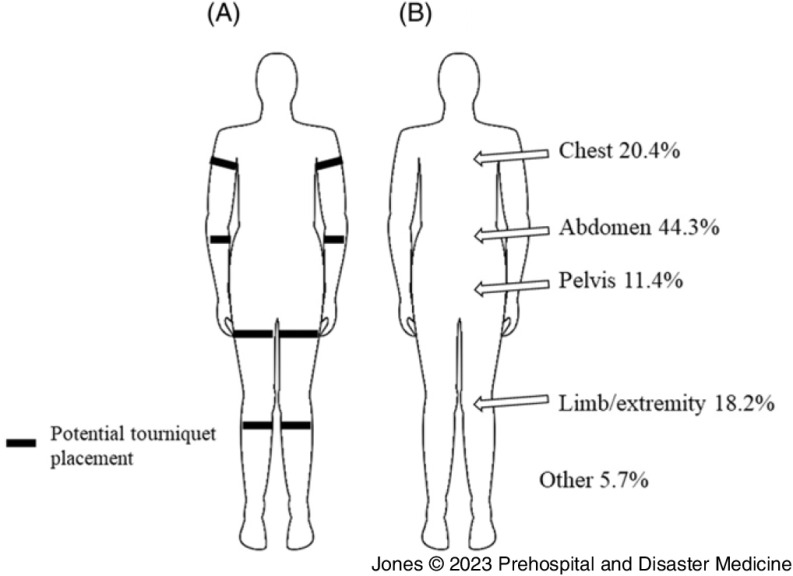
Results: Patients were primarily white (63.8%), male (80.3%), with a median age of 34 (IQR 24-51) years. Roughly one-half of patients experienced blunt (49.0%) versus penetrating (48.2%) injury. The most common types of blunt trauma were motor vehicle injuries (83.5%), followed by falls (9.3%), other (3.6%), assaults (1.8%), and incidents due to machinery (1.8%). The most common types of penetrating injuries were gunshot wounds (72.3%), stabbings (24.1%), other (2.1%), and impalements (1.5%). One-third of patients (34.5%) required some prehospital intervention, including intubation (77.4%), chest or needle decompression (18.8%), tourniquet (18.4%), and cardiopulmonary resuscitation (CPR; 5.6%). Sources of bleeding included the abdomen (44.3%), chest (20.4%), limb/extremity (18.2%), pelvis (11.4%), and other (5.7%). Patients waited for a median of six (IQR4-10) minutes for emergency responders to arrive at the scene of injury and traveled a median of 27 (IQR 19-42) minutes to an ED. Time to definitive care was a median of 57 (IQR 44-77) minutes, with a range of 12-232 minutes. Twenty-four-hour mortality was 15% (n = 100) with 81 patients dying due to exsanguination or hemorrhage.
Conclusion: Patients who experience critical injury may experience lengthy times to receipt of definitive care and may benefit from bystander action for hemorrhage control to improve patient outcomes.
Keywords: emergency treatments; hemorrhage; injury; trauma; wound.
Conflict of interest statement
The authors declare no conflicts of interest. This work was not financially supported.
Figures
References
-
- World Health Organization. Injuries and Violence 2021. https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence. Accessed November 18, 2021.
-
- Eastridge BJ, Holcomb JB, Shackelford S. Outcomes of traumatic hemorrhagic shock and the epidemiology of preventable death from injury. Transfusion. 2019;59(S2):1423–1428. - PubMed
-
- Joint Committee to Create a National Policy to Enhance Survivability from Mass Casualty Shooting Events; Jacobs LM, Eastman A, McSwain N, et al. Improving survival from active shooter events: The Hartford Consensus. Bull Am Coll Surg. 2015;100(1 Suppl):32–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
