

Underlying Causes of TIA and Minor Ischemic Stroke and Risk of Major Vascular Events
- PMID: 37782494
- PMCID: PMC10546292
- DOI: 10.1001/jamaneurol.2023.3344
Underlying Causes of TIA and Minor Ischemic Stroke and Risk of Major Vascular Events
Abstract
Importance: The coexistence of underlying causes in patients with transient ischemic attack (TIA) or minor ischemic stroke as well as their associated 5-year risks are not well known.
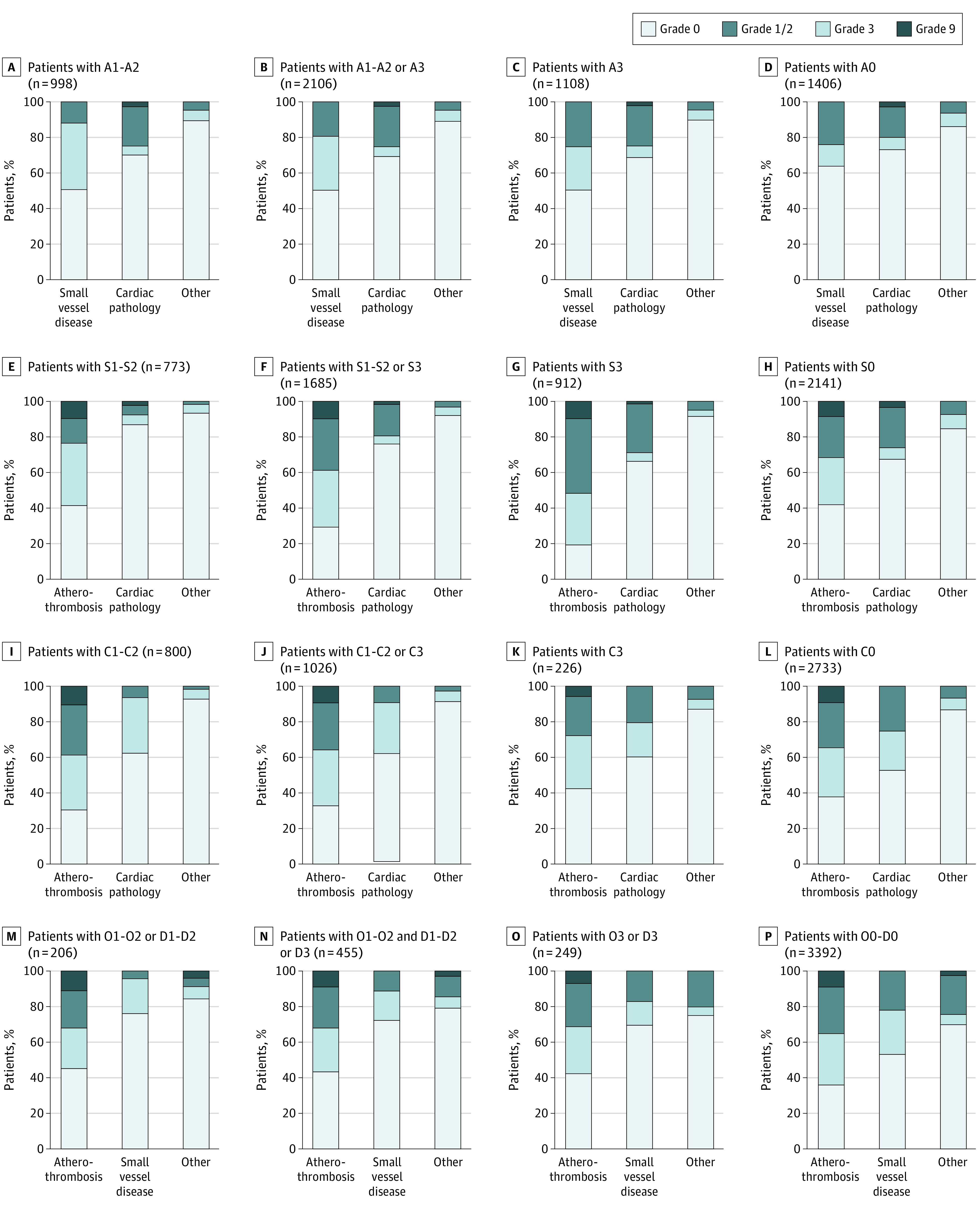
Objective: To apply the ASCOD (atherosclerosis, small vessel disease, cardiac pathology, other cause, or dissection) grading system to assess coexistence of underlying causes of TIA and minor ischemic stroke and the 5-year risk for major vascular events.
Design, setting, and participants: This international registry cohort (TIAregistry.org) study enrolled 4789 patients from June 1, 2009, to December 31, 2011, with 1- to 5-year follow-up at 61 sites in 21 countries. Eligible patients had a TIA or minor stroke (with modified Rankin Scale score of 0 or 1) within the last 7 days. Among these, 3847 patients completed the 5-year follow-up by December 31, 2016. Data were analyzed from October 1, 2022, to June 15, 2023.
Exposure: Five-year follow-up.
Main outcomes and measures: Estimated 5-year risk of the composite outcome of stroke, acute coronary syndrome, or cardiovascular death.
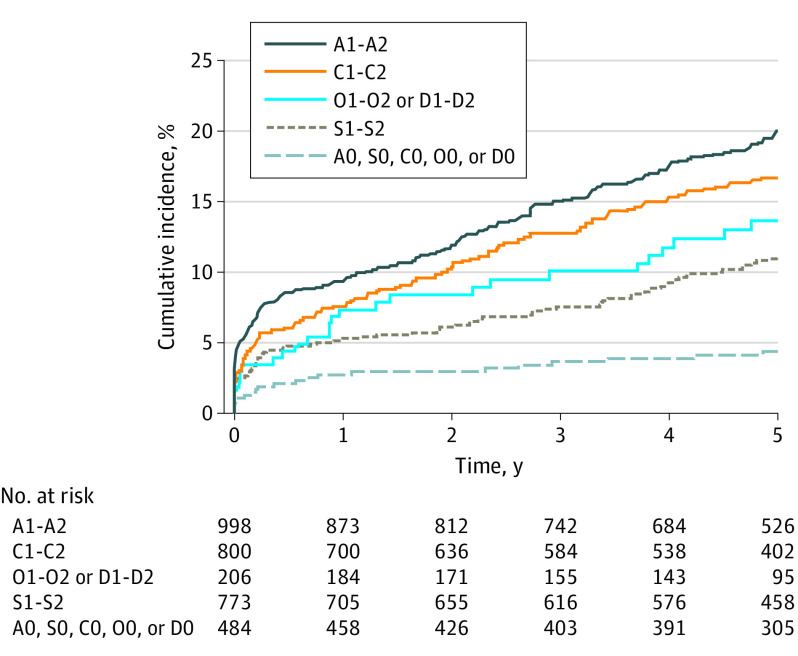
Results: A total of 3847 patients (mean [SD] age, 66.4 [13.2] years; 2295 men [59.7%]) in 42 sites were enrolled and participated in the 5-year follow-up cohort (median percentage of 5-year follow-up per center was 92.3% [IQR, 83.4%-97.8%]). In 998 patients with probable or possible causal atherosclerotic disease, 489 (49.0%) had some form of small vessel disease (SVD), including 110 (11.0%) in whom a lacunar stroke was also probably or possibly causal, and 504 (50.5%) had no SVD; 275 (27.6%) had some cardiac findings, including 225 (22.6%) in whom cardiac pathology was also probably or possibly causal, and 702 (70.3%) had no cardiac findings. Compared with patients with none of the 5 ASCOD categories of disease (n = 484), the 5-year rate of major vascular events was almost 5 times higher (hazard ratio [HR], 4.86 [95% CI, 3.07-7.72]; P < .001) in patients with causal atherosclerosis, 2.5 times higher (HR, 2.57 [95% CI, 1.58-4.20]; P < .001) in patients with causal lacunar stroke or lacunar syndrome, and 4 times higher (HR, 4.01 [95% CI, 2.50-6.44]; P < .001) in patients with causal cardiac pathology.
Conclusion and relevance: The findings of this cohort study suggest that in patients with TIA and minor ischemic stroke, the coexistence of atherosclerosis, SVD, cardiac pathology, dissection, or other causes is substantial, and the 5-year risk of a major vascular event varies considerably across the 5 categories of underlying diseases. These findings further suggest the need for secondary prevention strategies based on pathophysiology rather than a one-size-fits-all approach.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
