

Efficacy, safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir for HIV pre-exposure prophylaxis in transgender women: a secondary analysis of the HPTN 083 trial
- PMID: 37783219
- PMCID: PMC10842527
- DOI: 10.1016/S2352-3018(23)00200-X
Efficacy, safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir for HIV pre-exposure prophylaxis in transgender women: a secondary analysis of the HPTN 083 trial
Abstract
Background: The HIV Prevention Trials Network (HPTN) 083 trial showed that long-acting injectable cabotegravir was more effective than tenofovir disoproxil fumarate plus emtricitabine in preventing HIV in cisgender men and transgender women who have sex with men. We aimed to characterise the cohort of transgender women included in HPTN 083.
Methods: HPTN 083 is an ongoing, phase 2b/3, randomised, multicentre, double-blind, double-dummy clinical trial done at 43 sites in seven countries (Argentina, Brazil, Peru, the USA, South Africa, Thailand, and Viet Nam). HIV-negative participants were randomly assigned (1:1) to receive injectable cabotegravir or tenofovir disoproxil fumarate plus emtricitabine. The study design and primary outcomes of the blinded phase of HPTN 083 have already been reported. An enrolment minimum of 10% transgender women was set for the trial. Here we characterise the cohort of transgender women enrolled from Dec 6, 2016, to May 14, 2020, when the study was unblinded. We report sociodemographic characteristics, use of gender affirming hormone therapy, and behavioural assessments of the transgender women participants. Laboratory testing and safety evaluations are also reported. The trial is registered at ClinicalTrials.gov, NCT02720094.
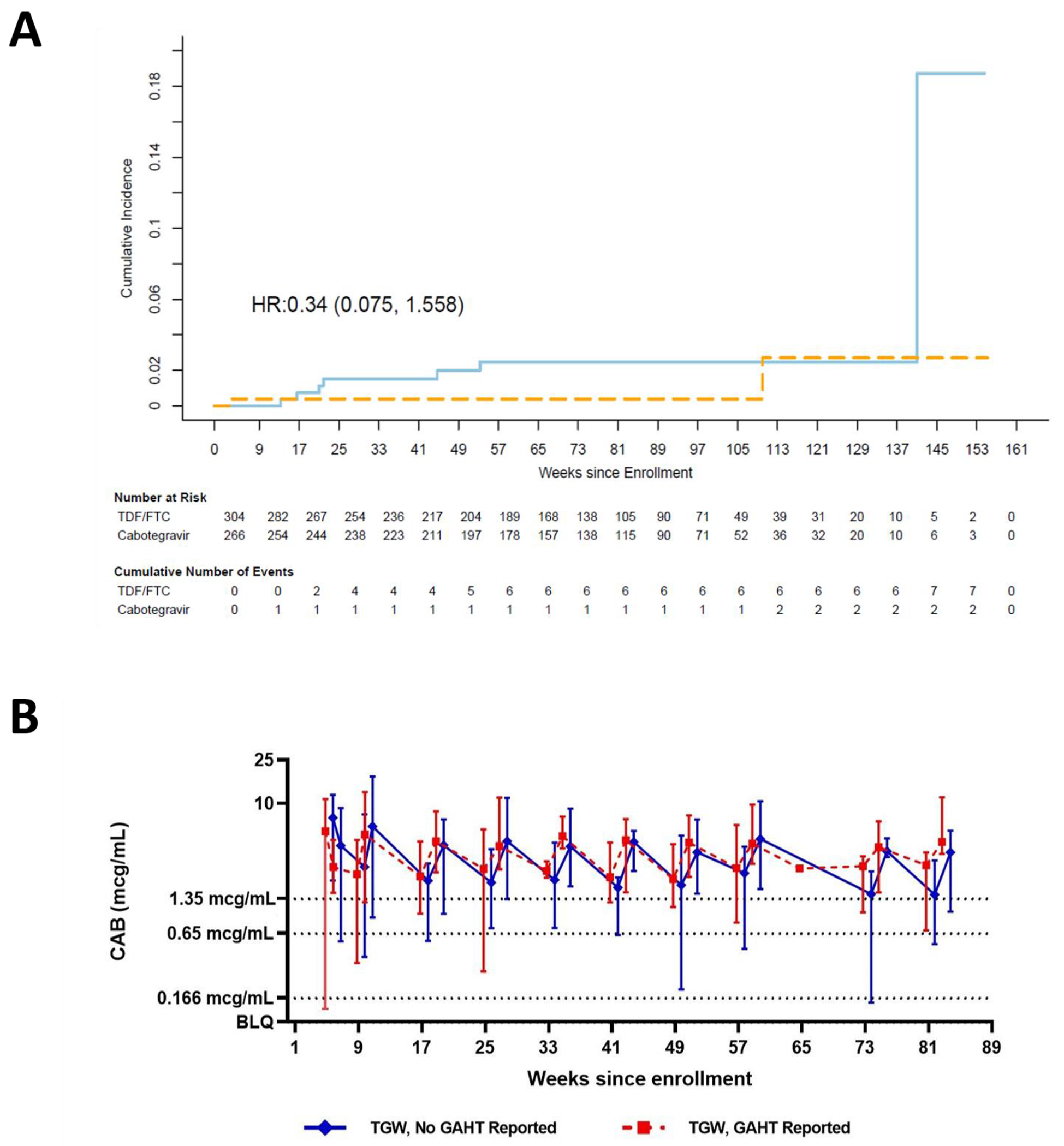
Findings: HPTN 083 enrolled 570 transgender women (304 tenofovir disoproxil fumarate plus emtricitabine; 266 injectable cabotegravir). Transgender women were primarily from Asia (225 [39%]) and Latin America (205 [36%]); 330 (58%) reported using gender affirming hormone therapy. Intimate partner violence was common (270 [47%] reported emotional abuse and 172 [30%] reported physical abuse) and 323 (57%) reported a history of childhood sexual abuse. 159 (28%) transgender women disagreed that they were at risk for HIV, and 142 (25%) screened positive for depressive symptoms. During study follow-up, incidence of syphilis was 16·25% (95% CI 13·28-19·69), rectal gonorrhoea was 11·66% (9·14-14·66), and chlamydia was 20·61% (17·20-24·49). Frequency of adverse events was similar between the treatment groups. Nine seroconversions occurred among transgender women during the blinded phase of the study (seven in the tenofovir disoproxil fumarate plus emtricitabine group and two in the injectable cabotegravir group); overall incidence was 1·19 per 100 person-years (95% CI 0·54-2·25): 1·80 per 100 person-years (0·73-3·72) in the tenofovir disoproxil fumarate plus emtricitabine group and 0·54 per 100 person-years (0·07-1·95) in the injectable cabotegravir group (hazard ratio 0·34 [95% CI 0·08-1·56]). Cabotegravir concentrations did not differ by gender affirming hormone therapy use.
Interpretation: HIV prevention strategies for transgender women cannot be addressed separately from social and structural vulnerabilities. Transgender women were well represented in HPTN 083 and should continue to be prioritised in HIV prevention studies. Our results suggest that injectable cabotegravir is a safe and effective pre-exposure prophylaxis option for transgender women.
Funding: National Institute of Allergy and Infectious Diseases and ViiV Healthcare.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests MAM has received grant funding from ViiV/GSK and Gilead Sciences for industry-sponsored research. RJL reports receiving study products and additional support for study conduct to sites from ViiV Healthcare and was given study products from Gilead Sciences during the conduct of the study. RJL received advisory scientific board fees, and travel support from Merck Inc outside the submitted work. JFR is a paid employee and stockholder of Gilead Sciences. ARR is a paid employee and stockholder of ViiV Healthcare. CP reports grants from the National Institutes of Health (NIH), advisory board fees from University of North Carolina at Chapel Hill, The Fenway Institute, and University of California, Los Angeles, outside the submitted work, and participated in data safety monitoring boards at University of North Carolina at Chapel Hill and Massachusetts General Hospital. JF reports grants from ViiV Healthcare UK and the National Institute of Allergy and Infectious Diseases, during the conduct of the study. SF was a paid employee and stockholder of GSK during the conduct of the study. MSC reports grants from NIH, scientific and medical advisory board fees, respectively, from Aerium and Atea, honoraria for lectures from MJH Life Sciences, Clinical Care Solutions, Virology Education, Amgen, Medscape, and UpToDate, and for an educational panel from Astra Zeneca. MSC reports travel support from GSK and was co-chair in the HIV Prevention Trials Network and COVID-19 Prevention Network. All other authors declare no competing interests.
Figures
Comment in
-
Optimising oral PrEP while awaiting long-acting cabotegravir.Lancet HIV. 2023 Nov;10(11):e694-e695. doi: 10.1016/S2352-3018(23)00231-X. Epub 2023 Sep 29. Lancet HIV. 2023. PMID: 37783220 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
