

Diagnostic criteria and etiopathogenesis of type 2 diabetes and its complications: Lessons from the Pima Indians
- PMID: 37783422
- PMCID: PMC10805453
- DOI: 10.1016/j.lpm.2023.104176
Diagnostic criteria and etiopathogenesis of type 2 diabetes and its complications: Lessons from the Pima Indians
Abstract
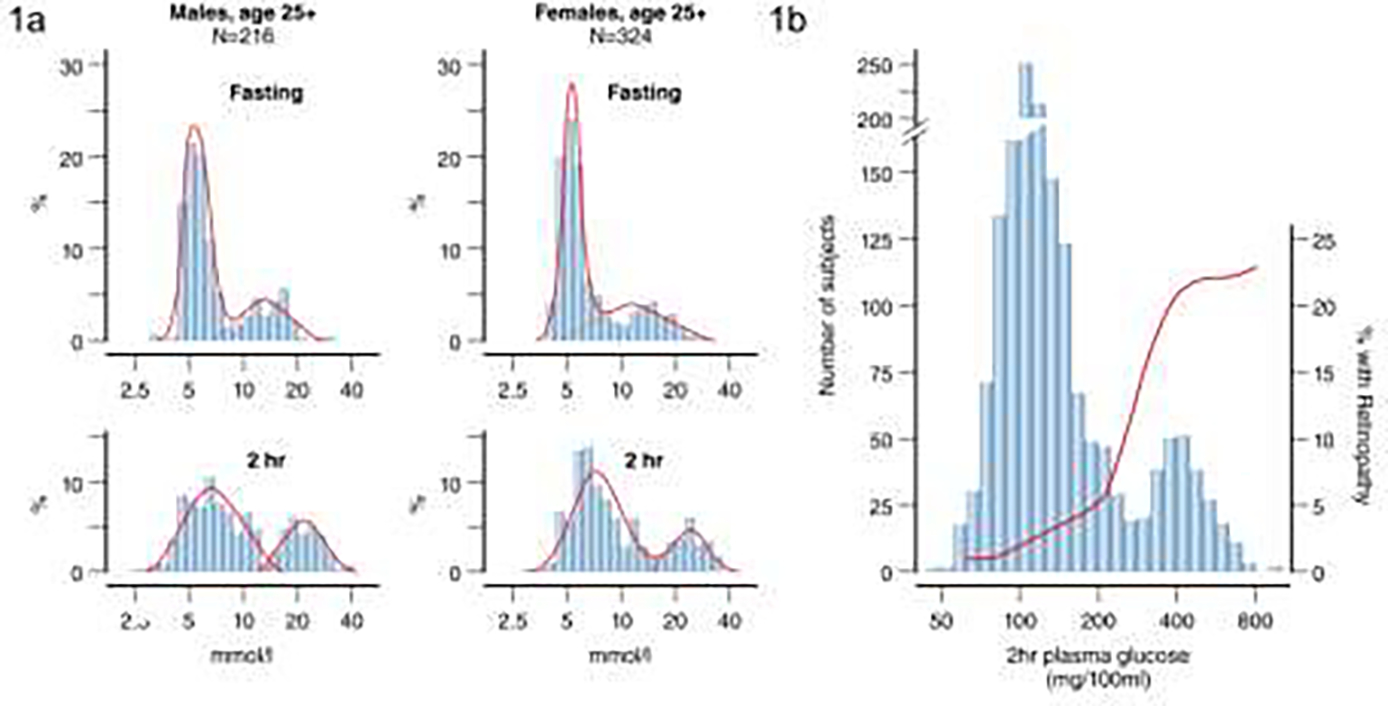
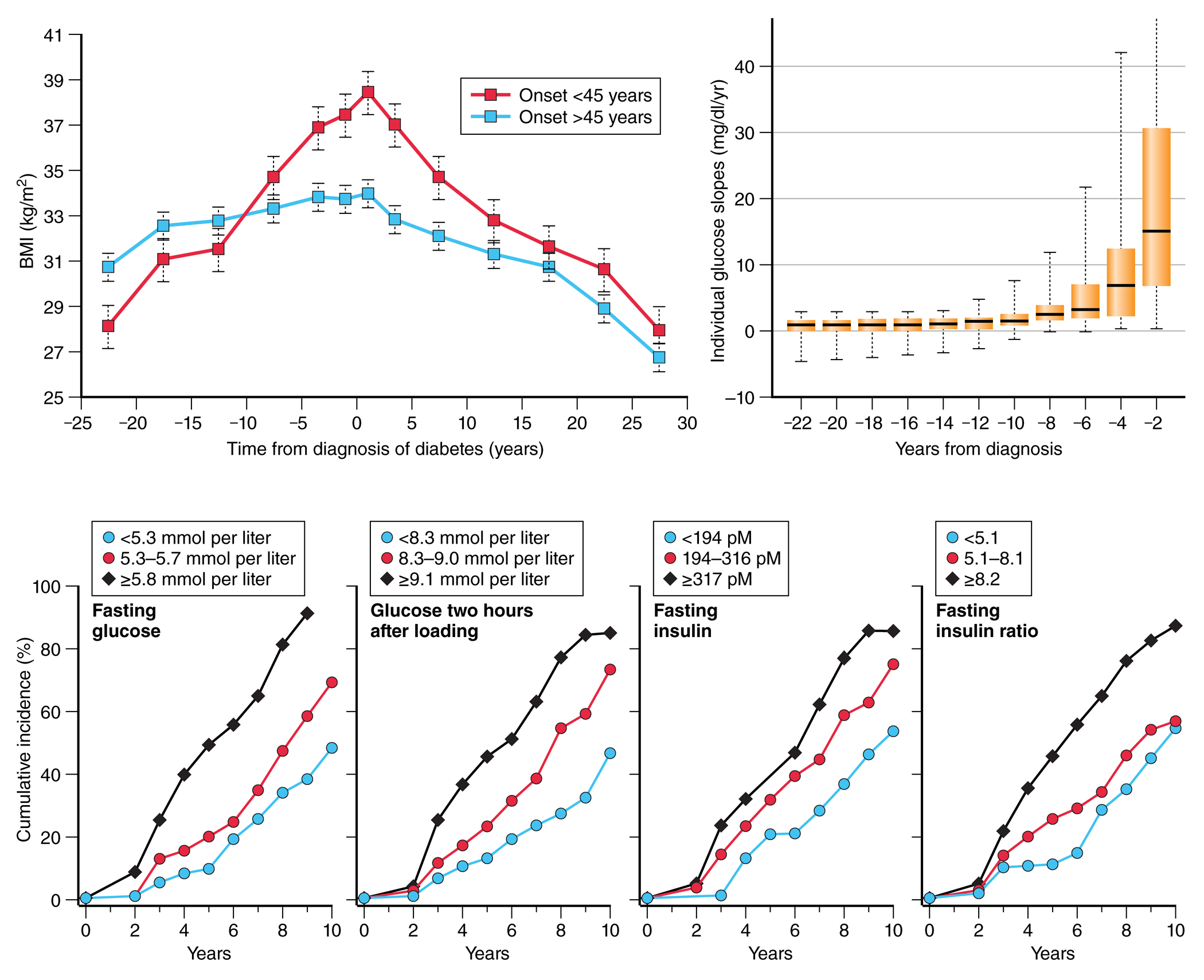
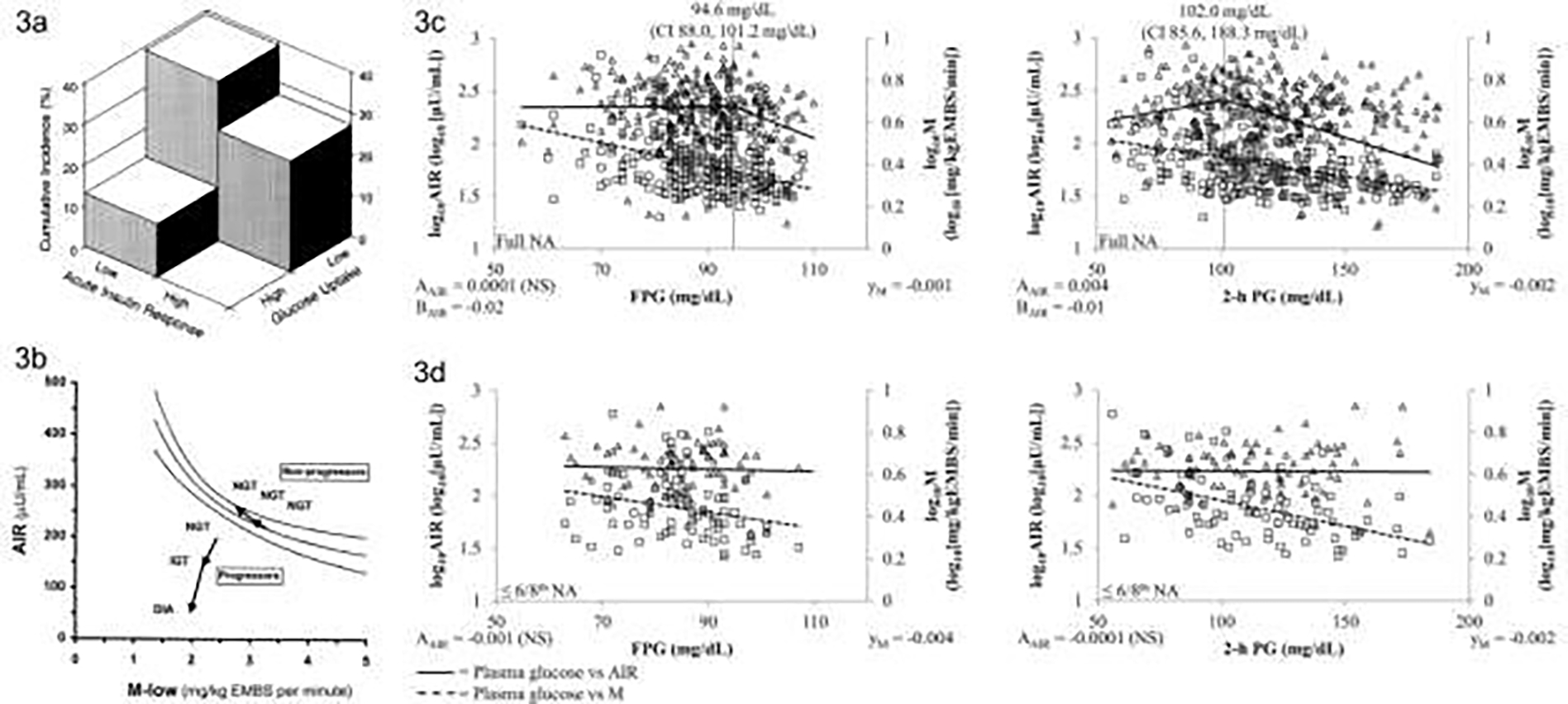
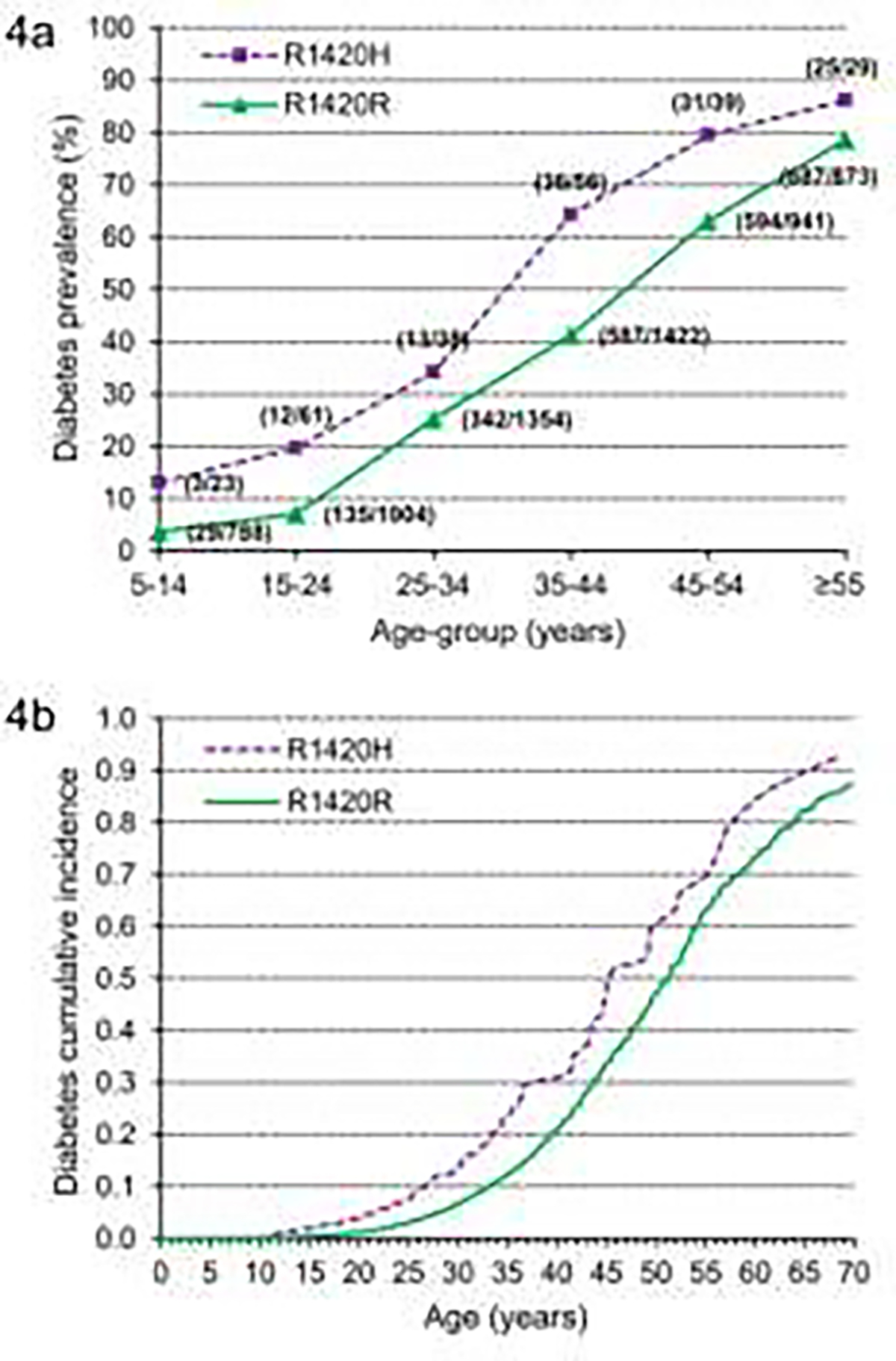
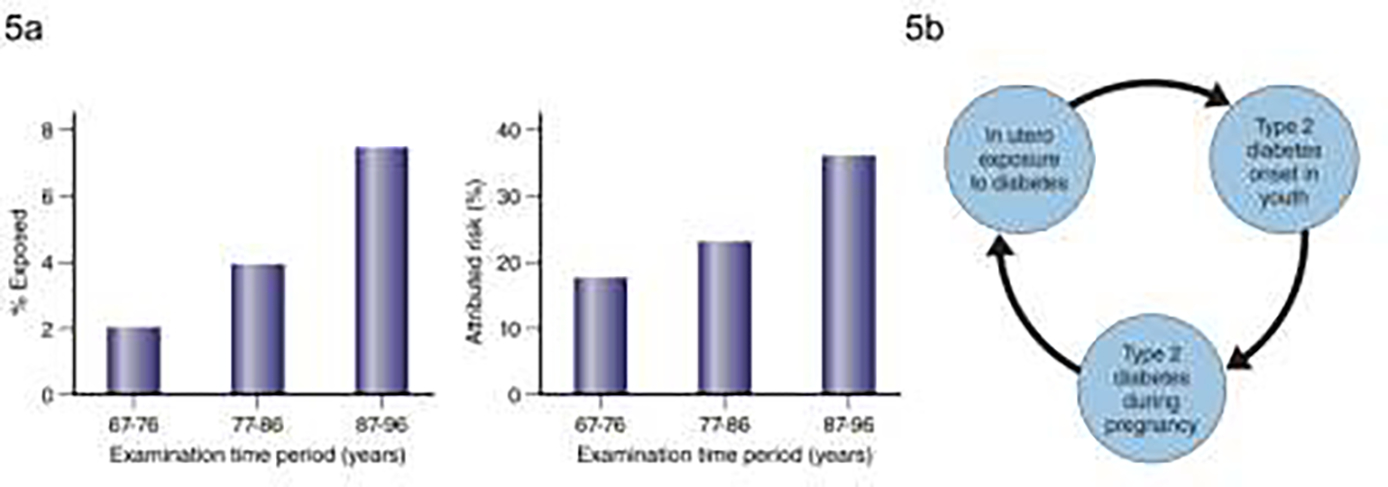
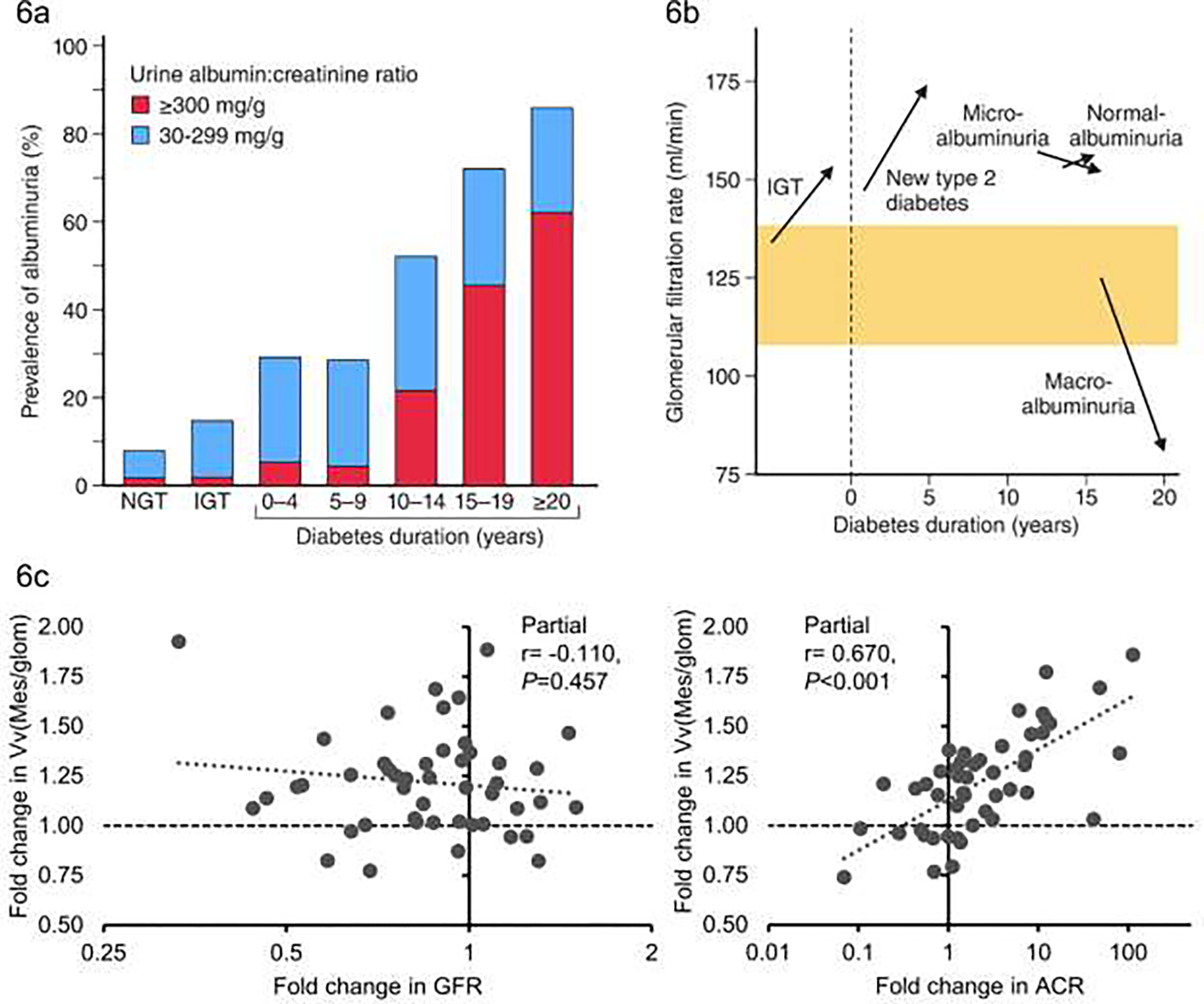
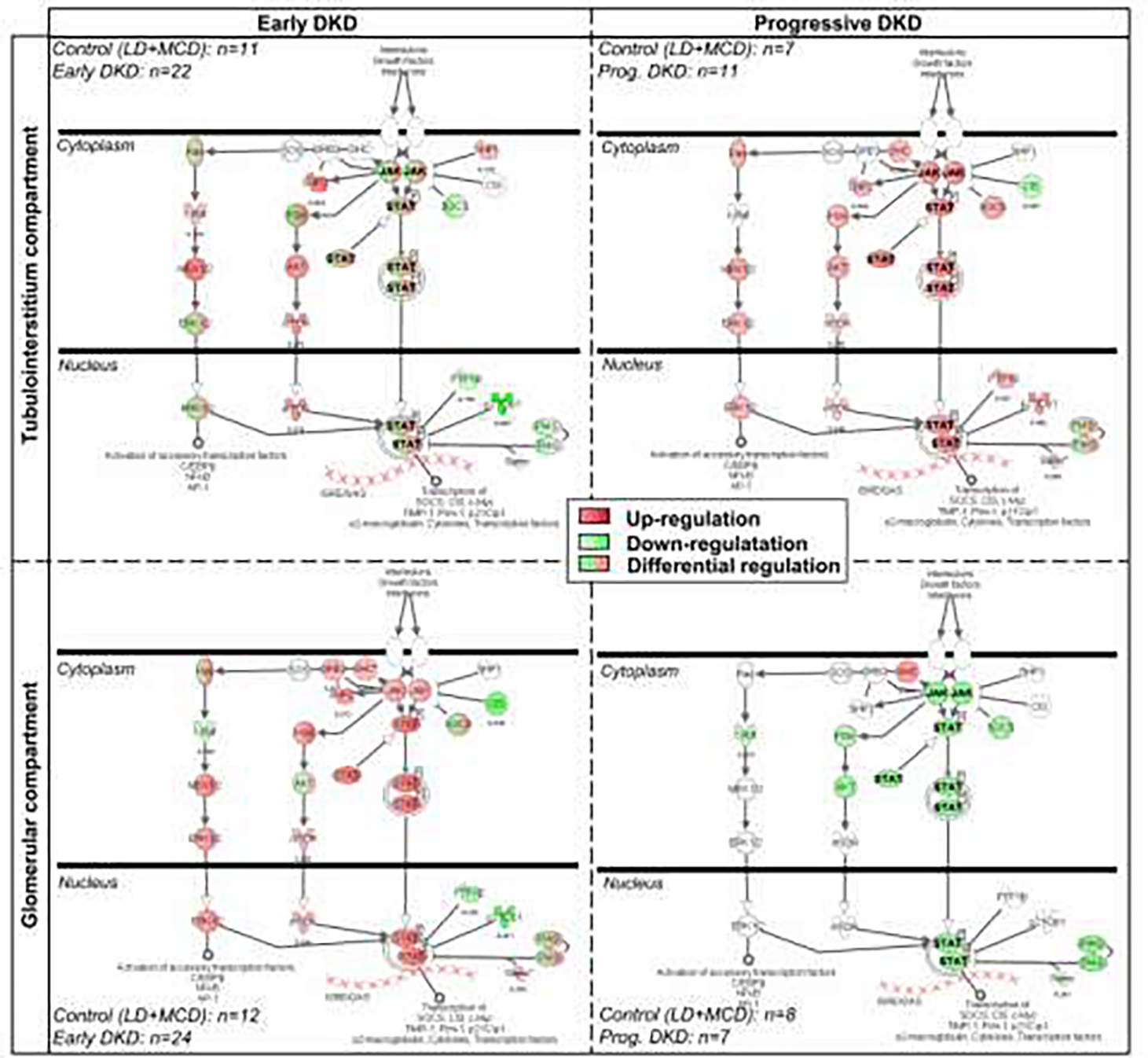
The Phoenix Epidemiology and Clinical Research Branch of the National Institute of Diabetes and Digestive and Kidney Diseases has conducted prospective studies of diabetes and its complications in the Pima Indians living in Arizona, USA for over 50 years. In this review we highlight areas in which these studies provided vital insights into the criteria used to diagnose type 2 diabetes, the pathophysiologic changes that accompany the development of type 2 diabetes, and the course and determinants of diabetes complications-focusing specifically on diabetic kidney disease. We include data from our longitudinal population-based study of diabetes and its complications, studies on the role of insulin resistance and insulin secretion in the pathophysiology of type 2 diabetes, and in-depth studies of diabetic kidney disease that include measures of glomerular function and research kidney biopsies. We also focus on the emerging health threat posed by youth-onset type 2 diabetes, which was first seen in the Pima Indians in the 1960s and is becoming an increasing issue worldwide.
Keywords: American Indians; Complications; Pathophysiology; Type 2 diabetes.
Published by Elsevier Masson SAS.
Conflict of interest statement
Disclosure of interest The authors declare that they have no competing interests.
Figures
Similar articles
-
Diabetic nephropathy in American Indians, with a special emphasis on the Pima Indians.Curr Diab Rep. 2008 Dec;8(6):486-93. doi: 10.1007/s11892-008-0083-1. Curr Diab Rep. 2008. PMID: 18990306 Free PMC article. Review.
-
Determinants of end-stage renal disease in Pima Indians with type 2 (non-insulin-dependent) diabetes mellitus and proteinuria.Diabetologia. 1993 Oct;36(10):1087-93. doi: 10.1007/BF02374503. Diabetologia. 1993. PMID: 8243859
-
Changing course of diabetic nephropathy in the Pima Indians.Diabetes Res Clin Pract. 2008 Nov 13;82 Suppl 1(Suppl 1):S10-4. doi: 10.1016/j.diabres.2008.09.014. Epub 2008 Oct 7. Diabetes Res Clin Pract. 2008. PMID: 18842316 Free PMC article. Review.
-
Effect of youth-onset type 2 diabetes mellitus on incidence of end-stage renal disease and mortality in young and middle-aged Pima Indians.JAMA. 2006 Jul 26;296(4):421-6. doi: 10.1001/jama.296.4.421. JAMA. 2006. PMID: 16868300
-
Diabetic renal disease in Pima Indians.Transplant Proc. 1989 Dec;21(6):3913-5. Transplant Proc. 1989. PMID: 2609404
Cited by
-
Young-Onset Diabetes in East Asians: From Epidemiology to Precision Medicine.Endocrinol Metab (Seoul). 2024 Apr;39(2):239-254. doi: 10.3803/EnM.2024.1968. Epub 2024 Apr 16. Endocrinol Metab (Seoul). 2024. PMID: 38626908 Free PMC article. Review.
-
A polygenic risk score derived from common variants of monogenic diabetes genes is associated with young-onset type 2 diabetes and cardiovascular-kidney complications.Diabetologia. 2025 Feb;68(2):367-381. doi: 10.1007/s00125-024-06320-3. Epub 2024 Nov 23. Diabetologia. 2025. PMID: 39579208 Free PMC article.
-
Prediabetes.Nat Rev Dis Primers. 2025 Jul 17;11(1):49. doi: 10.1038/s41572-025-00635-0. Nat Rev Dis Primers. 2025. PMID: 40676018 Review.
References
-
- Knowler WC, Bennett PH, Hamman RF, Miller M. Diabetes incidence and prevalence in Pima Indians: a 19-fold greater incidence than in Rochester, Minnesota. American journal of epidemiology 1978;108:497–505. - PubMed
-
- Knowler WC, Bennett PH, Bottazzo GF, Doniach D. Islet cell antibodies and diabetes mellitus in Pima Indians. Diabetologia 1979;17:161–4. - PubMed
-
- Savage PJ, Bennett PH, Senter RG, Miller M. High prevalence of diabetes in young Pima Indians: evidence of phenotypic variation in a genetically isolated population. Diabetes 1979;28:937–42. - PubMed
-
- Dabelea D, Palmer JP, Bennett PH, Pettitt DJ, Knowler WC. Absence of glutamic acid decarboxylase antibodies in Pima Indian children with diabetes mellitus. Diabetologia 1999;42:1265–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
