

Multifaceted analysis of cross-tissue transcriptomes reveals phenotype-endotype associations in atopic dermatitis
- PMID: 37783685
- PMCID: PMC10545679
- DOI: 10.1038/s41467-023-41857-8
Multifaceted analysis of cross-tissue transcriptomes reveals phenotype-endotype associations in atopic dermatitis
Abstract
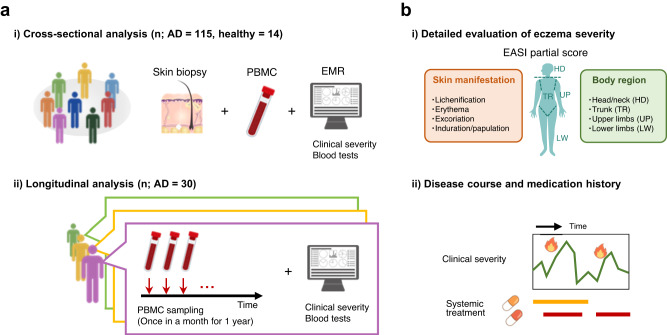
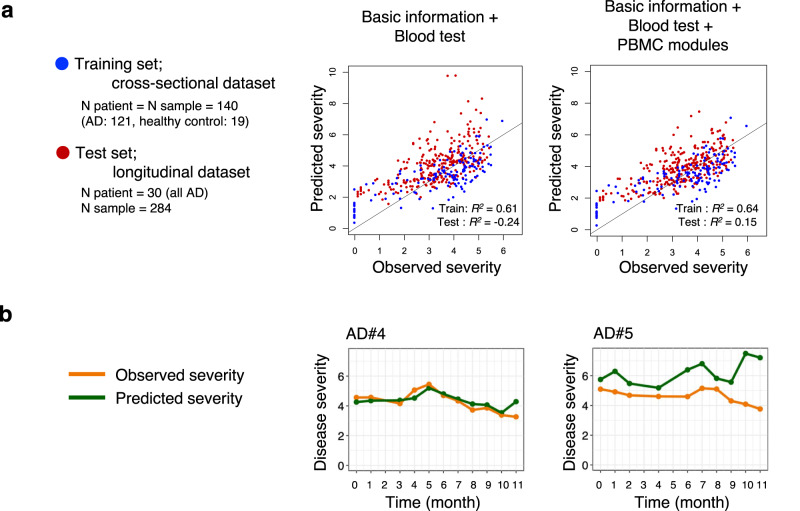
Atopic dermatitis (AD) is a skin disease that is heterogeneous both in terms of clinical manifestations and molecular profiles. It is increasingly recognized that AD is a systemic rather than a local disease and should be assessed in the context of whole-body pathophysiology. Here we show, via integrated RNA-sequencing of skin tissue and peripheral blood mononuclear cell (PBMC) samples along with clinical data from 115 AD patients and 14 matched healthy controls, that specific clinical presentations associate with matching differential molecular signatures. We establish a regression model based on transcriptome modules identified in weighted gene co-expression network analysis to extract molecular features associated with detailed clinical phenotypes of AD. The two main, qualitatively differential skin manifestations of AD, erythema and papulation are distinguished by differential immunological signatures. We further apply the regression model to a longitudinal dataset of 30 AD patients for personalized monitoring, highlighting patient heterogeneity in disease trajectories. The longitudinal features of blood tests and PBMC transcriptome modules identify three patient clusters which are aligned with clinical severity and reflect treatment history. Our approach thus serves as a framework for effective clinical investigation to gain a holistic view on the pathophysiology of complex human diseases.
© 2023. Springer Nature Limited.
Conflict of interest statement
H. Koseki has received research funds (grants paid to his institution) from Maruho and Kao. M.A. has received research support and funds (grants paid to his institution) from Maruho, Ono, Torii, Sato and Taiho. H. Kawasaki has received research funds (grants paid to his institution) from Torii. The rest of the authors declare no competing interests.
Figures






References
-
- Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387:1109–1122. - PubMed
-
- Yew YW, Thyssen JP, Silverberg JI. A systematic review and meta-analysis of the regional and age-related differences in atopic dermatitis clinical characteristics. J. Am. Acad. Dermatol. 2019;80:390–401. - PubMed
-
- Czarnowicki T, He H, Krueger JG, Guttman-Yassky E. Atopic dermatitis endotypes and implications for targeted therapeutics. J. Allergy Clin. Immunol. 2019;143:1–11. - PubMed
-
- Simpson EL, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N. Engl. J. Med. 2016;375:2335–2348. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
