

Superomedial-Posterior Pedicle-Based Reduction Mammaplasty: Evaluation of Effectiveness and BREAST-Q Outcomes of a Rapid and Safer Technique
- PMID: 37783863
- PMCID: PMC11150295
- DOI: 10.1007/s00266-023-03676-6
Superomedial-Posterior Pedicle-Based Reduction Mammaplasty: Evaluation of Effectiveness and BREAST-Q Outcomes of a Rapid and Safer Technique
Erratum in
-
Correction to: Aesthetic Plastic Surgery-Ethical Approval Corrections.Aesthetic Plast Surg. 2024 Nov;48(21):4599-4600. doi: 10.1007/s00266-024-04321-6. Aesthetic Plast Surg. 2024. PMID: 39207464 No abstract available.
Abstract
Introduction: Breast hypertrophy, a common pathological condition, often requires surgical intervention to alleviate musculoskeletal pain and improve patients' quality of life. Various techniques have been developed for breast reduction, each with its own advantages and complications. The primary aim of this study is to evaluate the efficacy, safety, and patient-reported outcomes of the authors technique: the Superomedial-Posterior Pedicle-Based Reduction Mammaplasty.
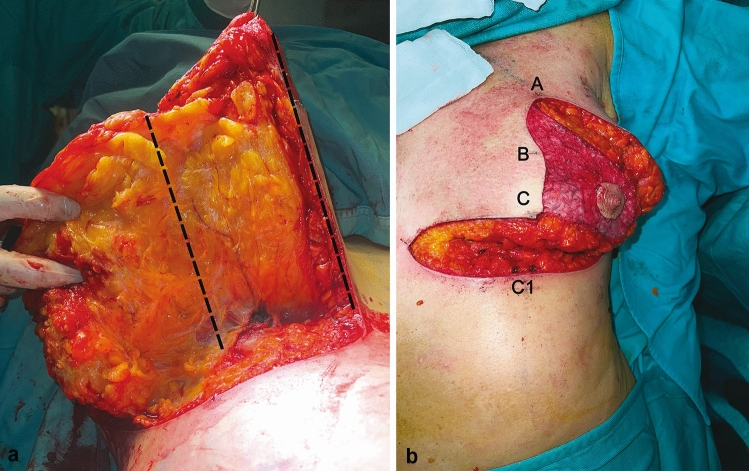
Material and methods: A prospective study was conducted on 912 patients who underwent breast reduction surgery between November 2012 and July 2020. The surgical technique involved preserving all glandular tissue from the areola to the pectoralis major muscle using the superomedial-posterior pedicle. The patients' demographic data, operative details, complications, breast-related quality of life (measured using the Breast-Q questionnaire), and nipple-areola complex sensitivity were analyzed.
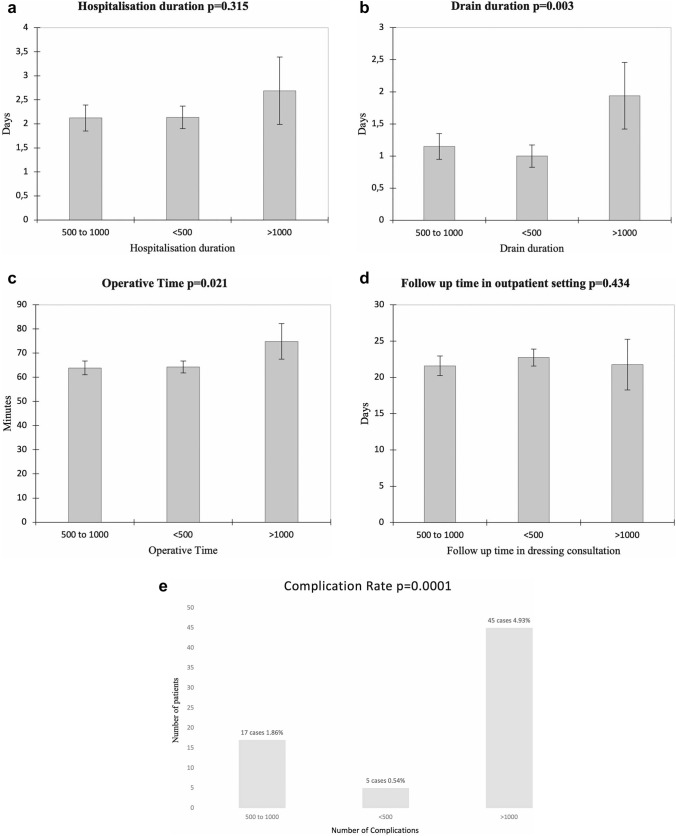
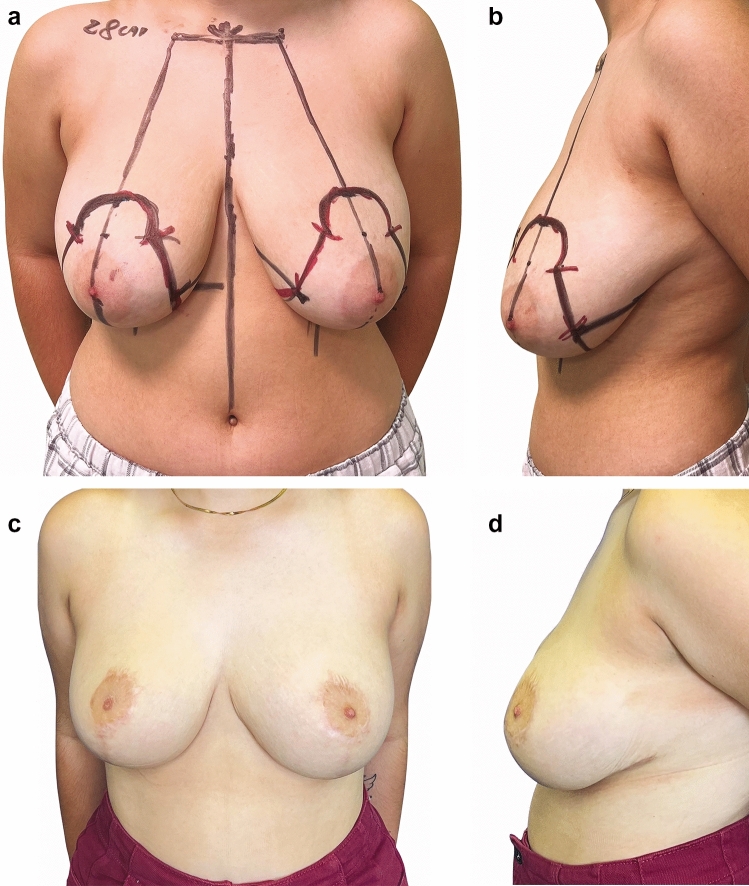
Results: The average operative time was 62.12 ± 10.3 minutes. Complications included minor wound dehiscence (4.05%) and hematoma (1.2%), with no cases of nipple-areola complex necrosis. Nipple-areola sensitivity was fully restored in all patients at the 2-year follow-up. Patient satisfaction with the procedure was high with a statistically significant difference observed between pre- and postoperative scores (p < 0.001) of the Breast-Q questionnaire.
Conclusion: Authors technique offers reliable vascularization and innervation of the nipple-areola complex and achieves satisfactory aesthetic outcomes. It is associated with shorter operative times compared to other techniques reported in the literature. The Superomedial-Posterior Pedicle-Based Reduction Mammaplasty represents a safe and effective method for breast reduction surgery, providing significant benefits to patients with breast hypertrophy.
Level of evidence i: This journal requires that authors assign a level of evidence to each article. For a full description of these evidence-based medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266 .
Keywords: Breast Q; Breast hypertrophy; Breast reduction mammoplasty; Nipple–areola complex (NAC) sensitivity; Operative time in breast reduction mammaplasty; Suction drains.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest to disclose.
Figures


References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
