

Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial
- PMID: 37783966
- PMCID: PMC10667093
- DOI: 10.1038/s41591-023-02568-1
Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial
Erratum in
-
Author Correction: Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial.Nat Med. 2024 Apr;30(4):1211. doi: 10.1038/s41591-024-02814-0. Nat Med. 2024. PMID: 38242983 Free PMC article. No abstract available.
Abstract
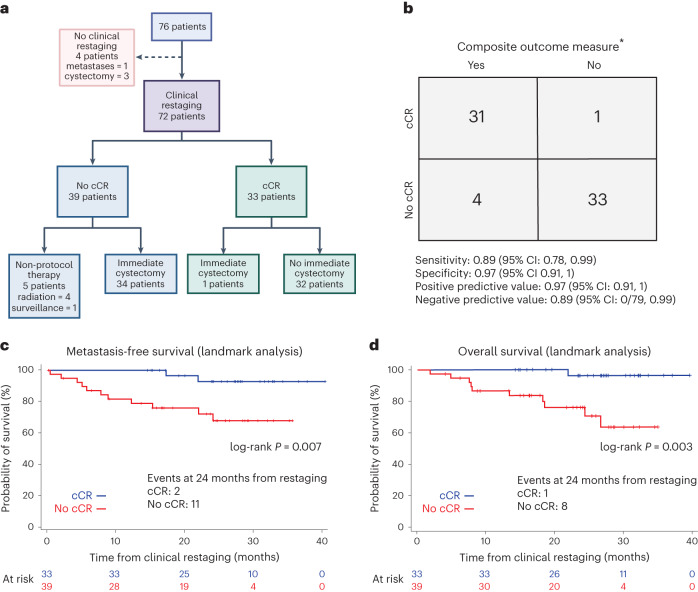
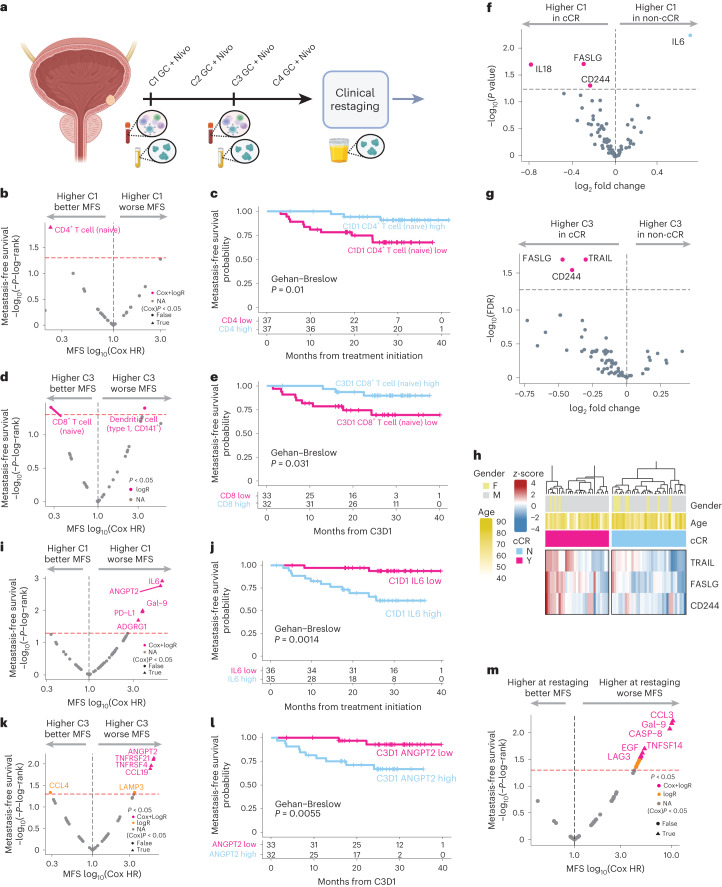
Cystectomy is a standard treatment for muscle-invasive bladder cancer (MIBC), but it is life-altering. We initiated a phase 2 study in which patients with MIBC received four cycles of gemcitabine, cisplatin, plus nivolumab followed by clinical restaging. Patients achieving a clinical complete response (cCR) could proceed without cystectomy. The co-primary objectives were to assess the cCR rate and the positive predictive value of cCR for a composite outcome: 2-year metastasis-free survival in patients forgoing immediate cystectomy or <ypT1N0 in patients electing immediate cystectomy. Seventy-six patients were enrolled; of these, 33 achieved a cCR (43%, 95% confidence interval (CI): 32%, 55%), and 32 of 33 who achieved a cCR opted to forgo immediate cystectomy. The positive predictive value of cCR was 0.97 (95% CI: 0.91, 1), meeting the co-primary objective. The most common adverse events were fatigue, anemia, neutropenia and nausea. Somatic alterations in pre-specified genes (ATM, RB1, FANCC and ERCC2) or increased tumor mutational burden did not improve the positive predictive value of cCR. Exploratory analyses of peripheral blood mass cytometry and soluble protein analytes demonstrated an association between the baseline and on-treatment immune contexture with clinical outcomes. Stringently defined cCR after gemcitabine, cisplatin, plus nivolumab facilitated bladder sparing and warrants further study. ClinicalTrials.gov identifier: NCT03451331 .
© 2023. The Author(s).
Conflict of interest statement
M.D.G. has received research funding from Bristol Myers Squibb, Novartis, Dendreon, AstraZeneca, Merck and Genentech. He has served as a consultant to Bristol Myers Squibb, Merck, Genentech, AstraZeneca, Pfizer, EMD Serono, SeaGen, Janssen, Numab, Dragonfly, GlaxoSmithKline, Basilea, UroGen, Rappta Therapeutics, Alligator, Silverback, Fujifilm, Curis, Gilead, Bicycle, Asieris, Abbvie and Analog Devices. S.D. has served as a consultant to Janssen, Ferring, Photocure, Taris, Pacific Edge, QED, Abbvie, Janssen, Bristol Myers Squibb, Sesen, Protara, Pfizer and CG Oncology. T.B.D. has served as a consultant to Astellas, AstraZeneca, Bayer, Janssen and Sanofi. R.M. has served as a consultant to Bristol Myers Squibb, Roche, Astellas and Seattle Genetics and has received research funding from Merck and Astellas. C.K. has served as a consultant to Exelixis, Sanofi, AVEO, EMD Serono and Janssen and has received research funding from Sanofi, Gilead Sciences, AstraZeneca, ESSA Pharma, Pionyr and Incyte. He owns stock in Biogen and Epic Systems. T.J. is an employee of Genentech. A.H. has served as a consultant to HTG Molecular Diagnostics and Immunorizon. L.W. is an employee of GeneDx. K.W.M. has served as a consultant to EMD Serono, Pfizer, UroGen and Riva Therapeutics, has received research support from Pfizer and Novo Ventures, has equity in Riva Therapeutics, has received writing fees from UpToDate and has received speaking fees from OncLive. He is named on an institutional patent filed on mutational signatures of DNA repair deficiency. N.B. has served as a consultant to Apricity, BreakBio, Carisma Therapeutics, CureVac, Genetech, Novartis, Primevax, Tempest Therapeutics, Dragonfly Therapeutics, BioNTech, Genotwin and Rome Therapeutics. She has received research support from Harbour Biomed Sciences and Regeneron. J.Z. is an employee of GeneDx. S.G. received research funding from Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Genentech, Regeneron and Takeda. J.S. has served as a consultant or advisor for Natera, Pacific Edge, Merck, Urogen and Janssen. S.K.P. has received travel support form CRISPR Therapeutics and Ipsen. All remaining authors declare no competing interests.
Figures







Comment in
-
Bladder-sparing neoadjuvant therapy for MIBC.Nat Rev Urol. 2023 Dec;20(12):703. doi: 10.1038/s41585-023-00832-0. Nat Rev Urol. 2023. PMID: 37914838 No abstract available.
References
-
- Griffiths G, Hall R, Sylvester R, Raghavan D, Parmar MK. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: long-term results of the BA06 30894 trial. J. Clin. Oncol. 2011;29:2171–2177. doi: 10.1200/JCO.2010.32.3139. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
