

Elranatamab in relapsed or refractory multiple myeloma: the MagnetisMM-1 phase 1 trial
- PMID: 37783970
- PMCID: PMC10579053
- DOI: 10.1038/s41591-023-02589-w
Elranatamab in relapsed or refractory multiple myeloma: the MagnetisMM-1 phase 1 trial
Abstract
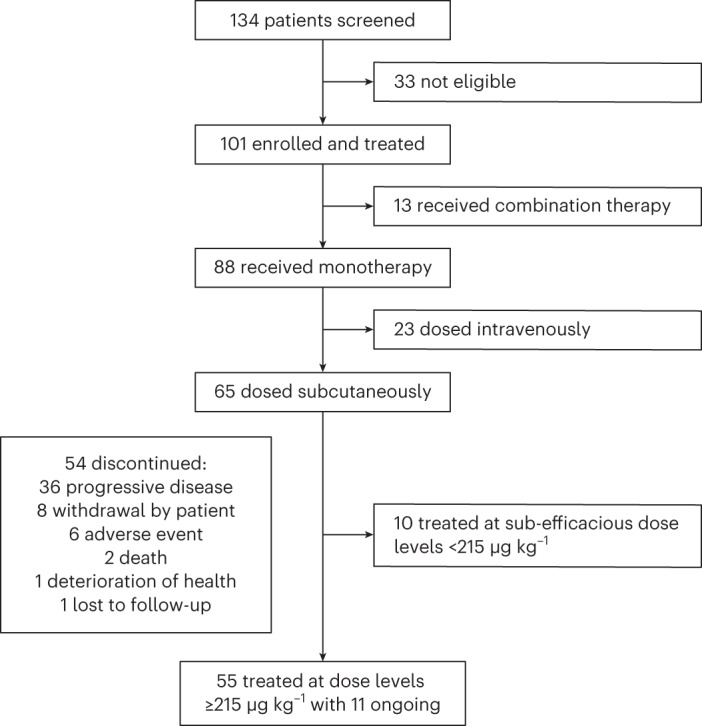
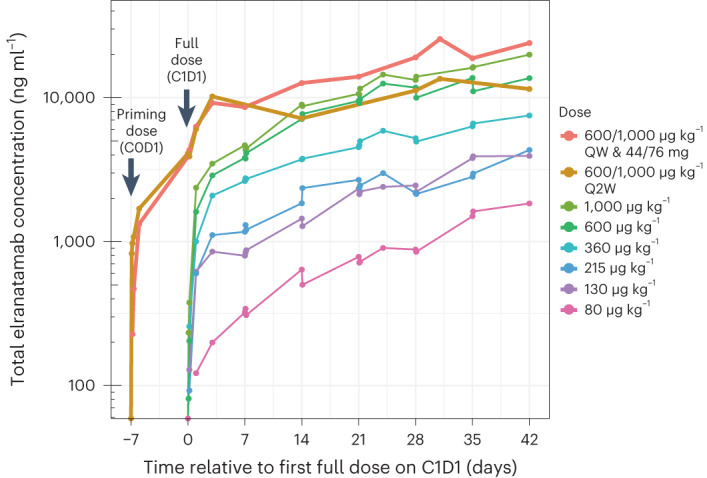
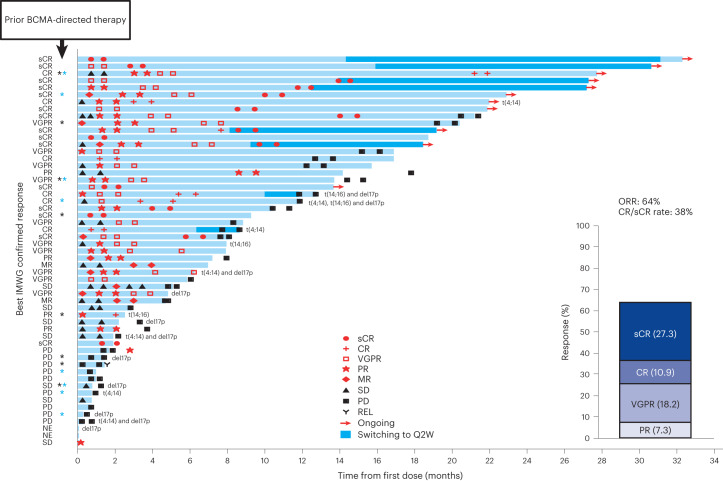
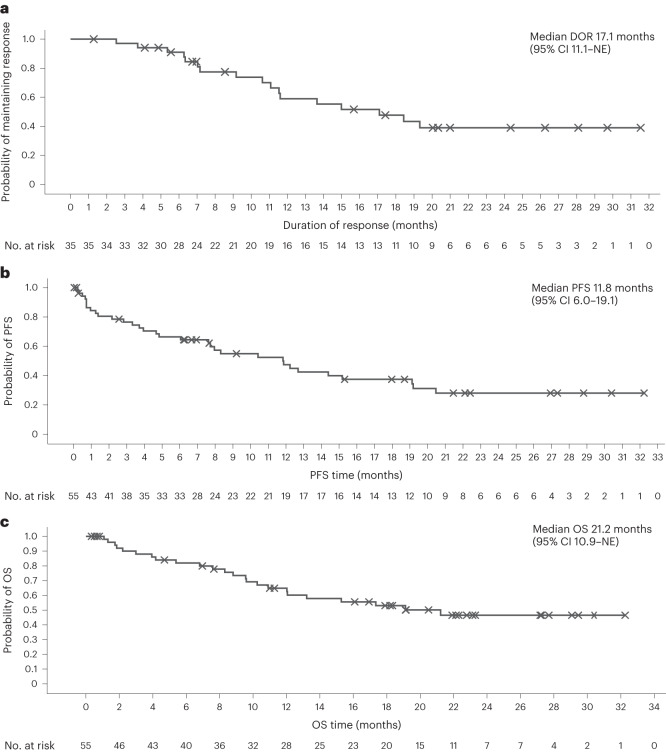
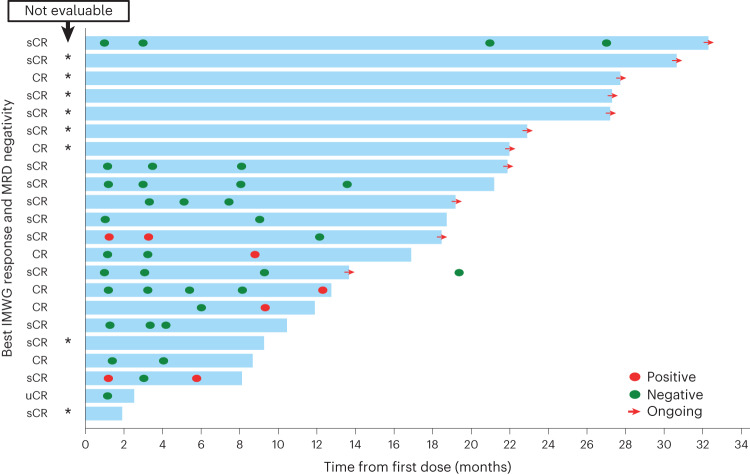
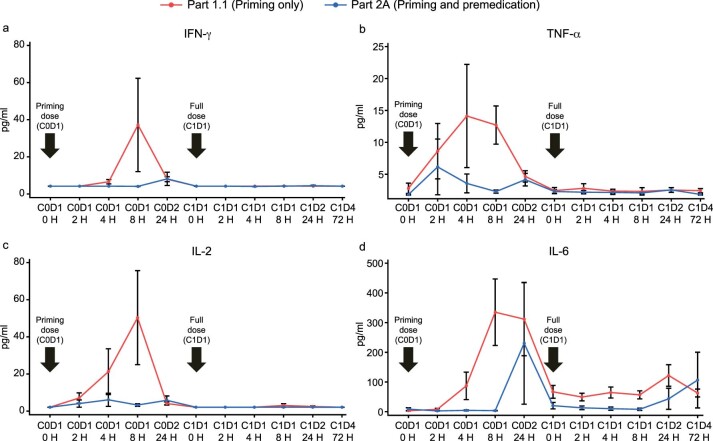
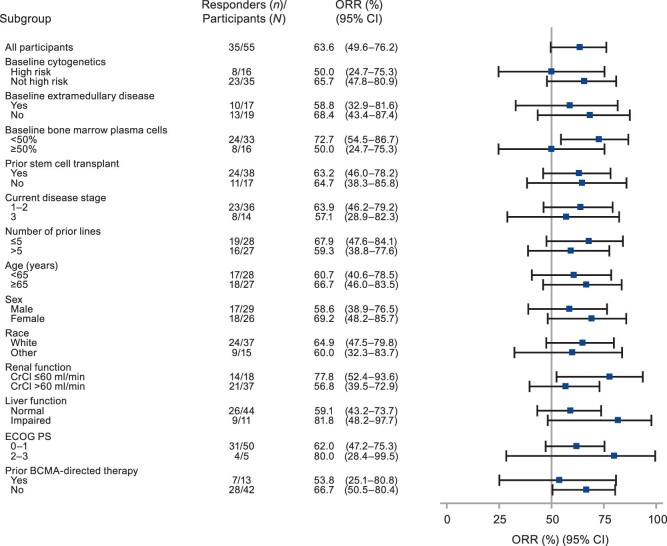
Multiple myeloma (MM) is a plasma cell malignancy expressing B cell maturation antigen (BCMA). Elranatamab, a bispecific antibody, engages BCMA on MM and CD3 on T cells. The MagnetisMM-1 trial evaluated its safety, pharmacokinetics and efficacy. Primary endpoints, including the incidence of dose-limiting toxicities as well as objective response rate (ORR) and duration of response (DOR), were met. Secondary efficacy endpoints included progression-free survival (PFS) and overall survival (OS). Eighty-eight patients with relapsed or refractory MM received elranatamab monotherapy, and 55 patients received elranatamab at efficacious doses. Patients had received a median of five prior regimens; 90.9% were triple-class refractory, 29.1% had high cytogenetic risk and 23.6% received prior BCMA-directed therapy. No dose-limiting toxicities were observed during dose escalation. Adverse events included cytopenias and cytokine release syndrome. Exposure was dose proportional. With a median follow-up of 12.0 months, the ORR was 63.6% and 38.2% of patients achieving complete response or better. For responders, the median DOR was 17.1 months. All 13 patients evaluable for minimal residual disease achieved negativity. Even after prior BCMA-directed therapy, 53.8% achieved response. For all 55 patients, median PFS was 11.8 months, and median OS was 21.2 months. Elranatamab achieved durable responses, manageable safety and promising survival for patients with MM. ClinicalTrials.gov Identifier: NCT03269136 .
© 2023. The Author(s).
Conflict of interest statement
N.J.B. received grant support from Celgene and Janssen; consulting fees from Janssen, Celgene, Amgen, Sanofi, Takeda, Pfizer and Karyopharm Therapeutics; and honoraria from Celgene, Janssen, AbbVie, Amgen, Sanofi, Takeda, Karyopharm Therapeutics, GlaxoSmithKline and Genentech/Roche. C.L.C. received grant support from Takeda, Celgene and Janssen and consulting fees and honoraria from Celgene, Janssen, Pfizer and Takeda. N.S.R. received grant support from Two Seventy Bio; consulting fees and honoraria from Amgen, Bristol Myers Squibb, Celgene, Janssen, Merck, GlaxoSmithKline and Takeda; and honoraria from Research to Practice and Medscape. M.Y.L. received grant support, consultancy and honoraria from AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Janssen, Karyopharm Therapeutics, Sanofi, Seattle Genetics and Takeda. B.D. received institutional grant support from Takeda, Janssen, Angiocrine, Pfizer, Poseida, Orca Bio, Molecular Template, Bristol Myers Squibb and MEI Pharma and consulting fees from Jazz Pharmaceuticals, Arivan Research and Gamida Cell. M.S. received grant support from ADCT Therapeutics and Partner Therapeutics; consulting fees and honoraria from Bristol Myers Squibb, Seattle Genetics and Pfizer; and honoraria from GlaxoSmithKline, Bristol Myers Squibb and Amgen. M.A.D., S.J., C.B., A.S. and E.M.C. are employed by Pfizer and hold stock or stock options in Pfizer. S.T. received grant support from Amgen, Bristol Myers Squibb, Genentech, GlaxoSmithKline, Janssen and Pfizer; consulting fees from Amgen, Bristol Myers Squibb and GlaxoSmithKline; and honoraria from Amgen, AstraZeneca, Bristol Myers Squibb, Janssen, Karyopharm Therapeutics, Pfizer, Sanofi and Takeda. A.J. received consulting fees and honoraria and holds membership on boards of directors or advisory committees for AbbVie, Amgen, Bristol Myers Squibb, Celgene, GlaxoSmithKline, Janssen, Karyopharm Therapeutics, Millennium, Sanofi, SkylineDx and Takeda. C.G. received grant support from Celgene; consulting fees and honoraria from Bristol Myers Squibb, Celgene and Janssen; and honoraria from Takeda. M.P.C. received grant support from Celgene and Bristol Myers Squibb and consulting fees and honoraria from Amgen, AstraZeneca, Celgene/Bristol Myers Squibb, Gilead, Janssen and Teva. M.S. received grant support from Janssen and consulting fees and honoraria from Bristol Myers Squibb, Takeda, Novartis, Karyopharm Therapeutics, Sanofi and Amgen. A.M.L. received institutional grant support from Bristol Myers Squibb, Genentech, Trillium Therapeutics, Sanofi, Pfizer and Janssen Oncology; consulting fees and honoraria from Bristol Myers Squibb, Pfizer and Trillium Therapeutics; honoraria from Bristol Myers Squibb, Genmab, Amgen and Janssen; and patents/royalties from Serametrix. M.H.T. and A.D. declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
